

The Tourniquet Ischemia Test Effectively Predicts the Efficacy of Lumbar Sympathetic Block in Patients with Lower Extremity Complex Regional Pain Syndrome Type 1
- PMID: 35698569
- PMCID: PMC9188397
- DOI: 10.2147/JPR.S365954
The Tourniquet Ischemia Test Effectively Predicts the Efficacy of Lumbar Sympathetic Block in Patients with Lower Extremity Complex Regional Pain Syndrome Type 1
Abstract
Background: Neuropathic pain is the most common clinical sign of complex regional pain syndrome (CRPS). Currently, lumbar sympathetic block (LSB) is commonly utilized in lower extremity CRPS that has failed to respond to medication therapy and physical therapy, but its effectiveness is unknown. The tourniquet ischemia test (IT) can distinguish between two types of CRPS: IT-positive CRPS and IT-negative CRPS.
Objective: The aim of the study was to investigate whether LSB improves pain scores in patients with lower extremity CRPS-1 and to screen factors to predict its efficacy.
Study design: Prospective clinical observational study.
Setting: Pain management center.
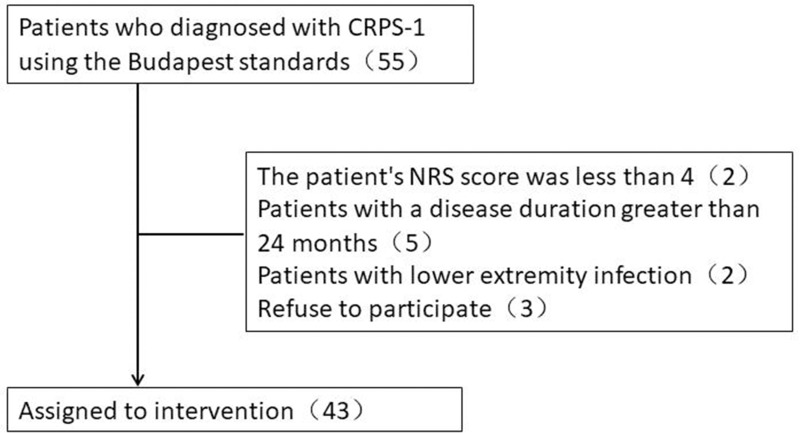
Subjects: Forty-three patients diagnosed with lower extremity CRPS-1 using the Budapest criteria were included as participants.
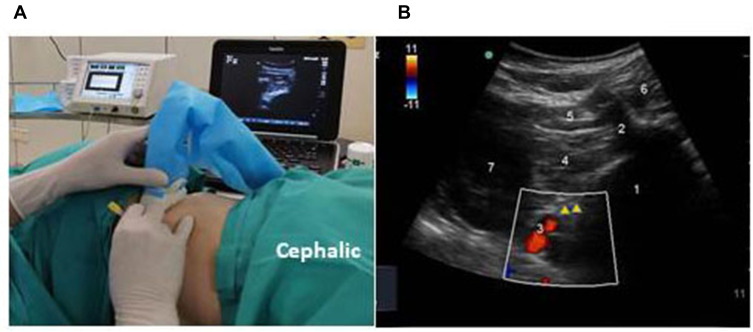
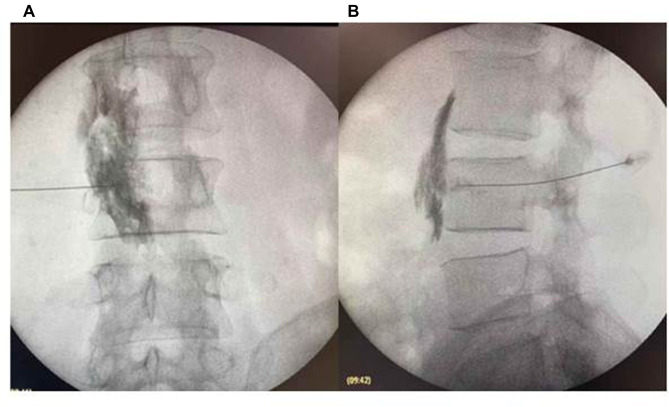
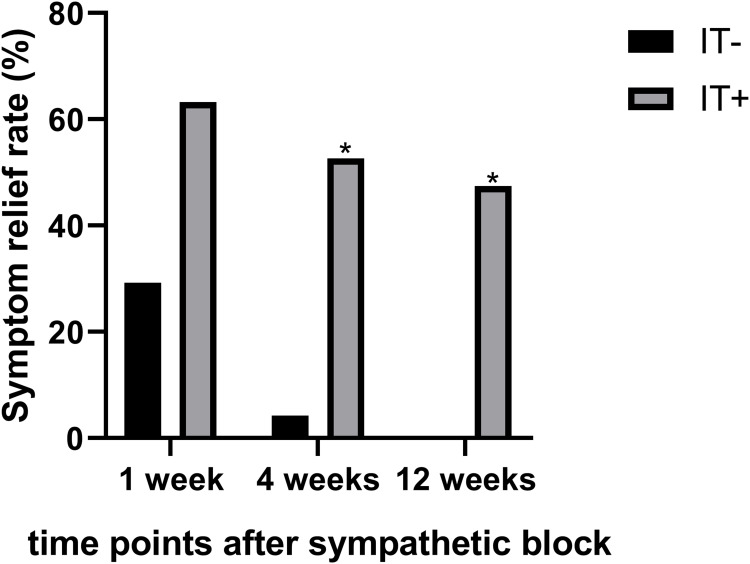
Methods: Forty-three CRPS-1 patients were treated with LSB therapy, and all of them underwent a tourniquet ischemia test (IT) before undergoing LSB therapy. LSB therapy was performed using a combination of ultrasonography and fluoroscopy. Then, numeric rating scale (NRS) scores and the symptom relief rates of patients were evaluated at 1, 4, and 12 weeks. Finally, peripheral blood inflammatory cytokine samples were collected before and after the LSB treatment.
Results: At 4 weeks after the treatment, the total effective symptom relief rate of LSB on CRPS-1 was 25.6% (11/43), with 52.6% (10/19) of IT(+) patients and 4.2% (1/24) of IT(-) patients. There was a significant difference between the IT(-) and IT(+) groups (P = 0.001). The multivariate binary logistic regression analysis revealed that the response to the tourniquet IT was the only significant independent predictor of sympathetic block success (p = 0.007).
Conclusion: Tourniquet IT is a simple, safe and effective test to distinguish patients with lower extremity CRPS-1. The response to the tourniquet IT is a reliable predictor of LSB effectiveness in lower extremity CRPS-1 patients.
Keywords: complex regional pain syndrome; lumbar sympathetic block; predict; tourniquet ischemia test.
© 2022 Xu et al.
Conflict of interest statement
All authors report no conflicts of interest in this work.
Figures
References
-
- de Mos M, de Bruijn AG, Huygen FJ, Dieleman JP, Stricker BH, Sturkenboom MC. The incidence of complex regional pain syndrome: a population-based study. Pain. 2007;129:12–20. - PubMed
-
- Kessler A, Yoo M, Calisoff R. Complex regional pain syndrome: an updated comprehensive review. NeuroRehabilitation. 2020;47:253–264. - PubMed
-
- Iolascon G, Moretti A. Pharmacotherapeutic options for complex regional pain syndrome. J Med. 2019;20:1377–1386. - PubMed
LinkOut - more resources
Full Text Sources
