

Efficacy and Safety of Masitinib in Corticosteroid-Dependent Severe Asthma: A Randomized Placebo-Controlled Trial
- PMID: 35698580
- PMCID: PMC9188333
- DOI: 10.2147/JAA.S337284
Efficacy and Safety of Masitinib in Corticosteroid-Dependent Severe Asthma: A Randomized Placebo-Controlled Trial
Abstract
Background: Masitinib is an oral tyrosine kinase inhibitor that selectively targets mast cell activity and platelet-derived growth factor receptor (PDGFR) signaling, both of which are implicated in various mechanisms of asthma pathogenesis.
Objective: Assessment of masitinib as an add-on to standard maintenance therapy as compared with placebo in the treatment of oral corticosteroid-dependent severe asthma.
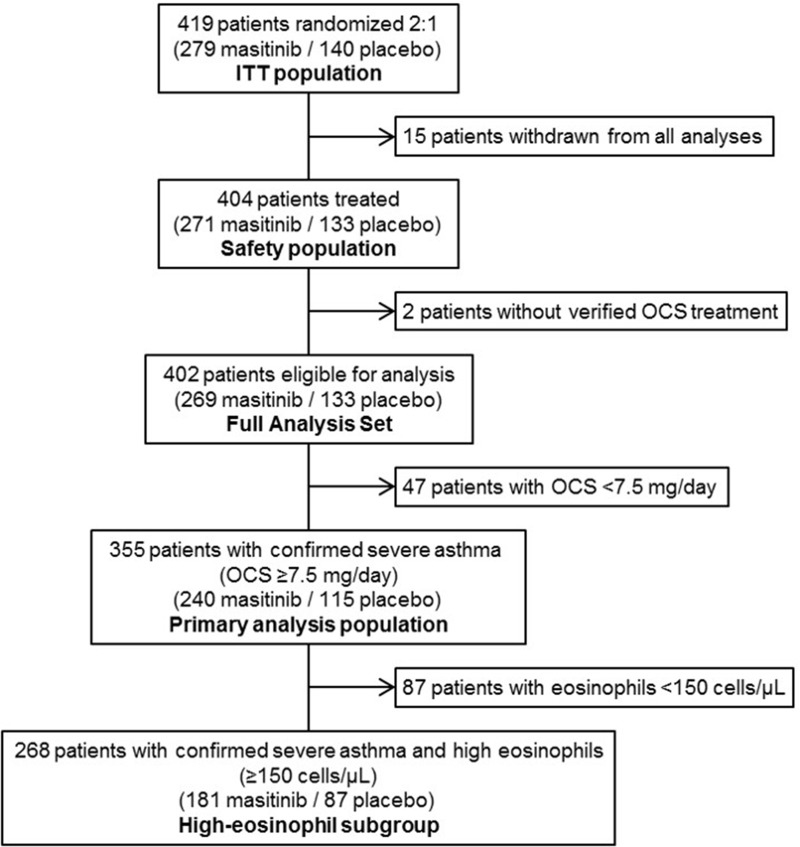
Methods: We conducted a randomized (2:1), placebo-controlled study of masitinib (6 mg/kg/d) in adults with severe asthma uncontrolled by high dose inhaled corticosteroids and long-acting beta-adrenoreceptor agonists plus oral corticosteroids (OCS) (≥7.5 mg/d). No minimum baseline blood eosinophil count was specified. Following a protocol amendment, the primary endpoint was reduction of annualized severe asthma exacerbation rate adjusted for the overall time on treatment (SAER). Subgroup analysis according to yearly cumulative OCS intake was also performed, a higher OCS dose indicating more severe asthma that is harder to control.
Results: Following an average exposure of approximately 13 months, masitinib (n = 240) reduced the SAER by 35% relative to placebo (n = 115) (rate ratio (RR) 0.65 (95% CI [0.47-0.90]; P = 0.010)). For patients with eosinophil ≥150 cell/µL, masitinib (n = 181) reduced SAER by 38% relative to placebo (n = 87); RR 0.62 (95% CI [0.42-0.91]; P = 0.016). Benefit of masitinib was shown to increase in the most severely affected patients (OCS intake of >1000 mg/year), with a significant (P < 0.01) reduction in SAER of 50%-70%. Safety was consistent with the known masitinib profile.
Conclusion: Orally administered masitinib reduces the risk of asthma exacerbations in severe asthma patients, with an acceptable safety profile. Masitinib may potentially provide a new treatment option for oral corticosteroid-dependent severe asthma.
Keywords: asthma clinical trials; asthma medication; mast cells; severe asthma; tyrosine kinases.
© 2022 Davidescu et al.
Conflict of interest statement
AM, OH and CDM are employees and shareholders of AB Science. AM reports patents WO2004/014903 issued to AB Science, PCT/EP2020/084251 pending to AB Science, US9078894B2 issued to AB Science, WO2003002106A2 issued to AB Science. PC reports grants/research support from Almirall, Boston Scientific, Boehringer Ingelheim, Centocor, GlaxoSmithKline, AstraZeneca, Novartis, and Teva; honoraria or consultation fees from Almirall, Boehringer Ingelheim, Johnson & Johnson, GlaxoSmithKline, Merck Sharp & Dohme, AstraZeneca, Novartis, Teva, Chiesi, Sanofi, AMU, SNCF, Centocor, Boston Scientific and ALK; served on advisory committees for Almirall, Boehringer Ingelheim, Johnson & Johnson, GlaxoSmithKline, AstraZeneca, Novartis, Teva, Chiesi, Schering Plough, and Sanofi. EI reports personal fees, non-financial support from AB Science, during the conduct of the study; and grants from AstraZeneca (Destination), Avillion - Mandala/Denali, Circassia, Gossamer Bio, NIH-SARP4, Novartis, PCORI; Personal fees for royalties or licenses from Wolters Kluwer; Consulting fees from Allergy and Asthma Network, Amgen, Arrowhead Pharmaceuticals, AstraZeneca, Avillion, Biometry, Equillium, Genentech, GlaxoSmithKline, Merck, NHLBI (CONNECTS), Novartis, Pneuma Respiratory, PPS Health, Regeneron, Sanofi Genzyme, Sienna Biopharmaceuticals, TEVA, Cowen; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events for Westchester Medical Center, Yale School of Medicine. Payment for expert testimony: Cambridge Medical Experts, Danaher Lagnese, SettlePou; Non-financial supports from Circassia (Equipment for PCORI-PREPARE Study), Genentech (Study Drug for NIH-Funded Study (PARK)), TEVA (Study Drug for PCORI-PREPARE Study), GSK (Background study medication for NIH PrecISE Trial); Data Safety Monitoring Board or Advisory Board for Novartis; Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid for NAEPP: National Asthma Education Prevention Program (Member, Coordinating Committee; Unpaid) Stock or stock options: Vorso (Stock Options; Unpaid). All remaining authors have no competing interests in this work.
Figures
References
-
- Global Initiative for Asthma. Global strategy for asthma management and prevention; 2020. Available from www.ginasthma.org. Accessed May 23, 2022.
-
- Mukherjee M, Forero DF, Tran S, et al. Sub-optimal treatment response to anti-IL-5 monoclonal antibodies in severe eosinophilic asthmatics with airway autoimmune phenomena [published online ahead of print, 2020 May 22]. Eur Respir J. 2020;56(4):2000117. doi: 10.1183/13993003.00117-2020 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
