

Variation in Out-of-Hospital Cardiac Arrest Survival Across Emergency Medical Service Agencies
- PMID: 35698973
- PMCID: PMC9233095
- DOI: 10.1161/CIRCOUTCOMES.121.008755
Variation in Out-of-Hospital Cardiac Arrest Survival Across Emergency Medical Service Agencies
Abstract
Background: Although studies have reported variation in out-of-hospital cardiac arrest (OHCA) survival by geographic location, little is known about variation in OHCA survival at the level of emergency medical service (EMS) agencies-which may have modifiable practices, unlike counties and regions. We quantified the variation in OHCA survival across EMS agencies and explored whether variation in 2 specific EMS resuscitation practices were associated with survival to hospital admission.
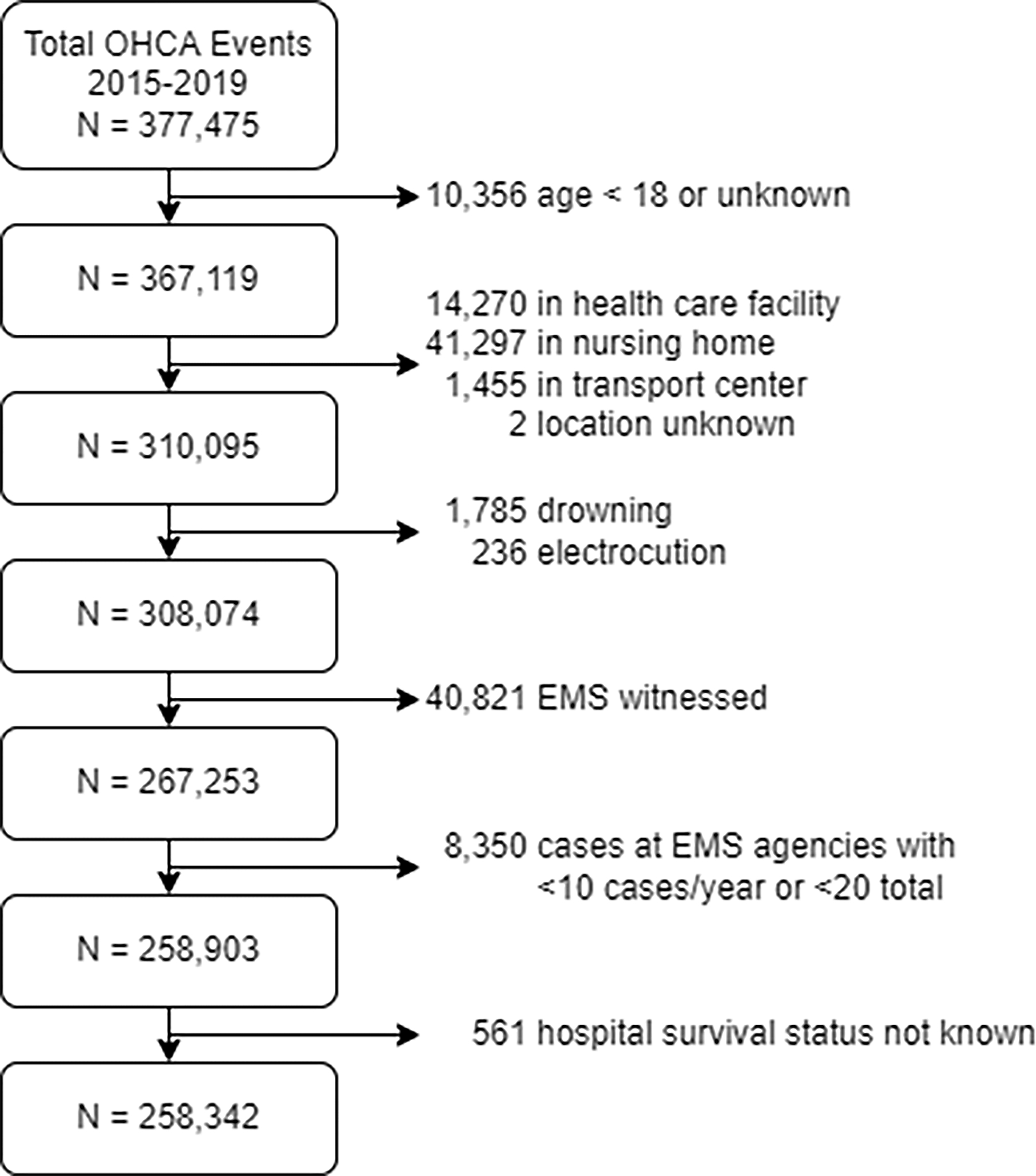
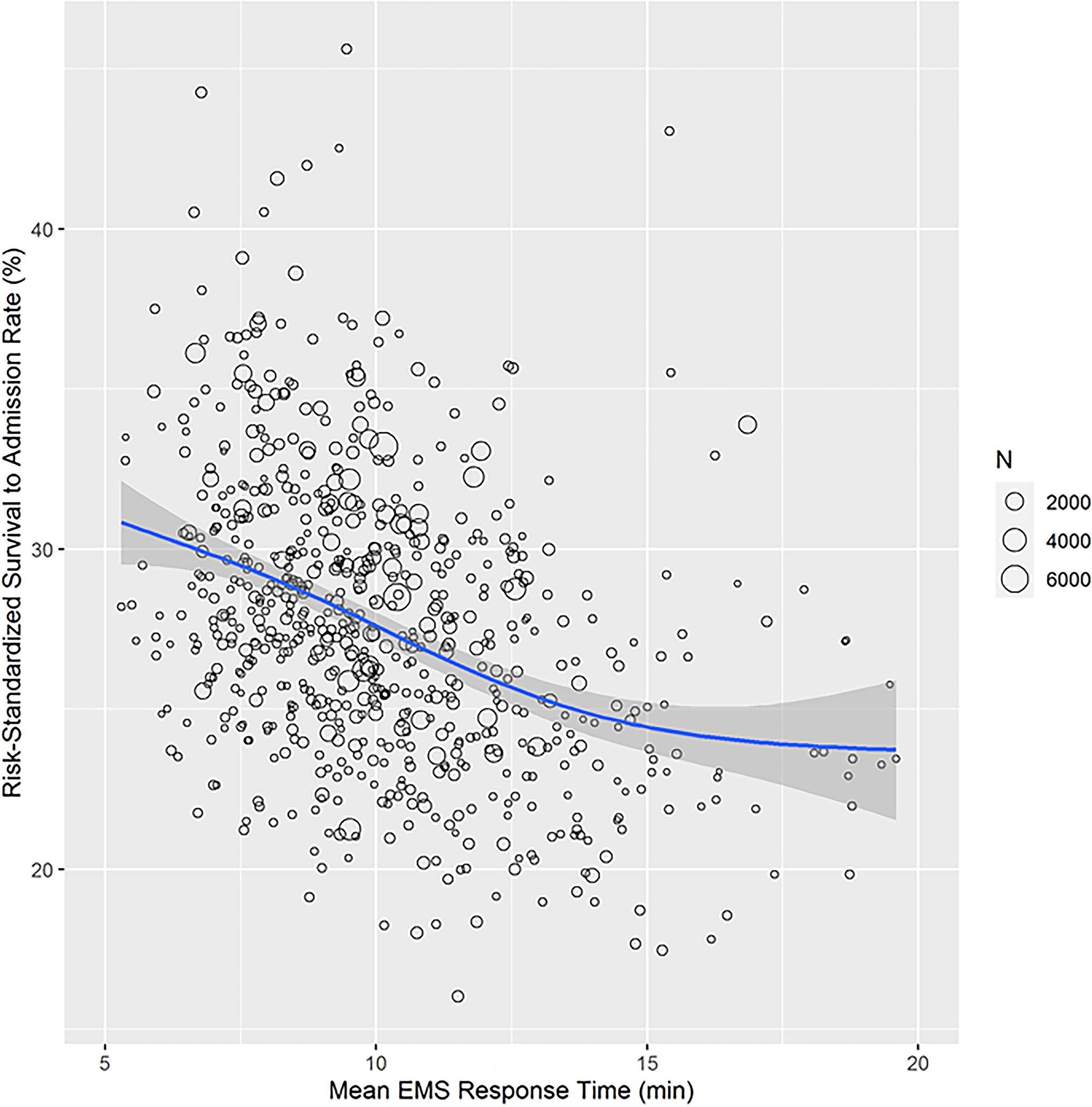
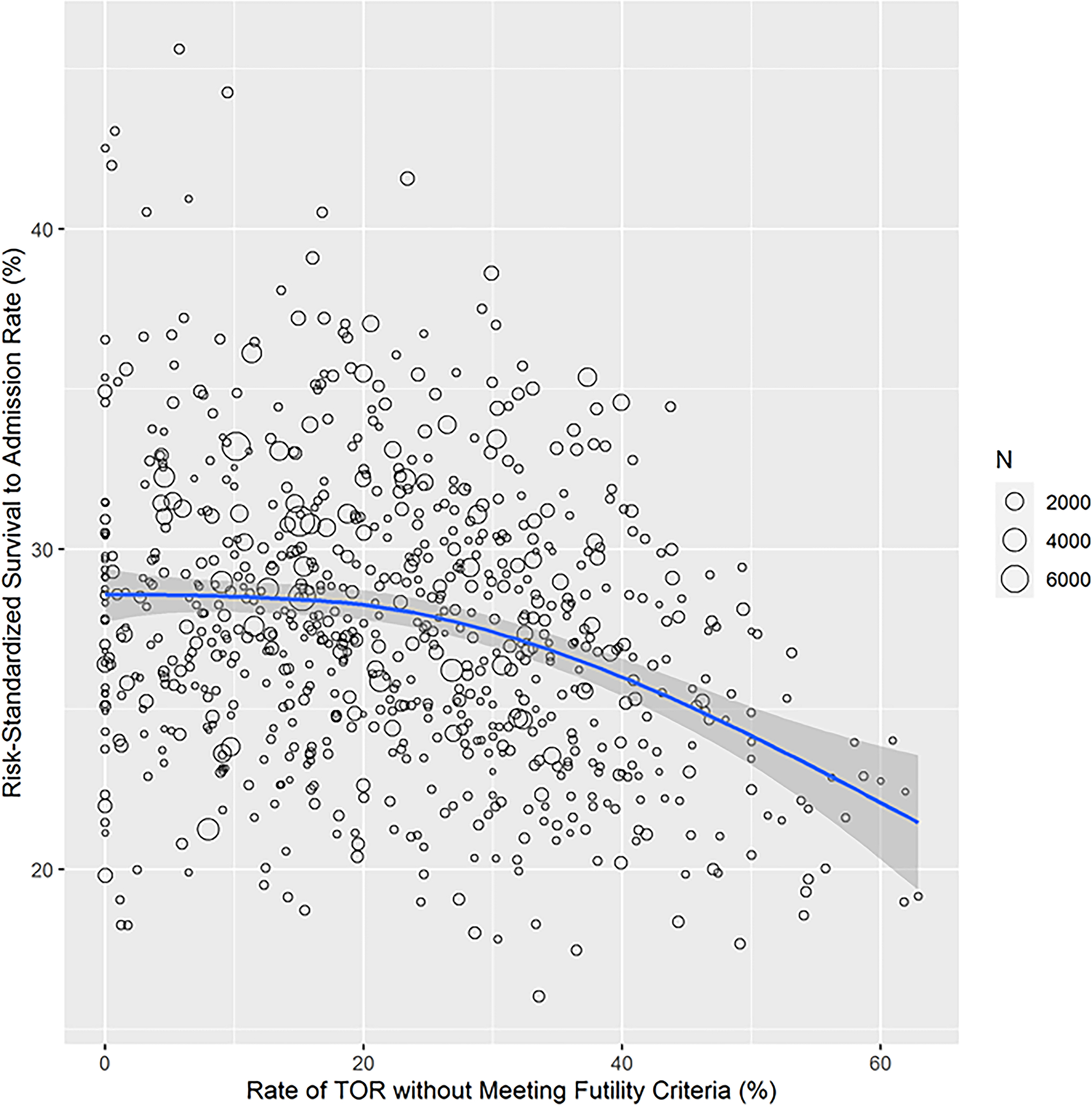
Methods: Within the Cardiac Arrest Registry to Enhance Survival, a prospective registry representing ≈51% of the US population, we identified 258 342 OHCAs from 764 EMS agencies with >10 OHCA cases annually during 2015 to 2019. Using hierarchical logistic regression, risk-standardized rates of survival to hospital admission were computed for each EMS agency. We quantified inter-agency variation in survival with median odds ratios and assessed the association of 2 resuscitation practices (EMS response time and the proportion of OHCAs with termination of resuscitation without meeting futility criteria) with EMS agency survival rates to hospital admission.
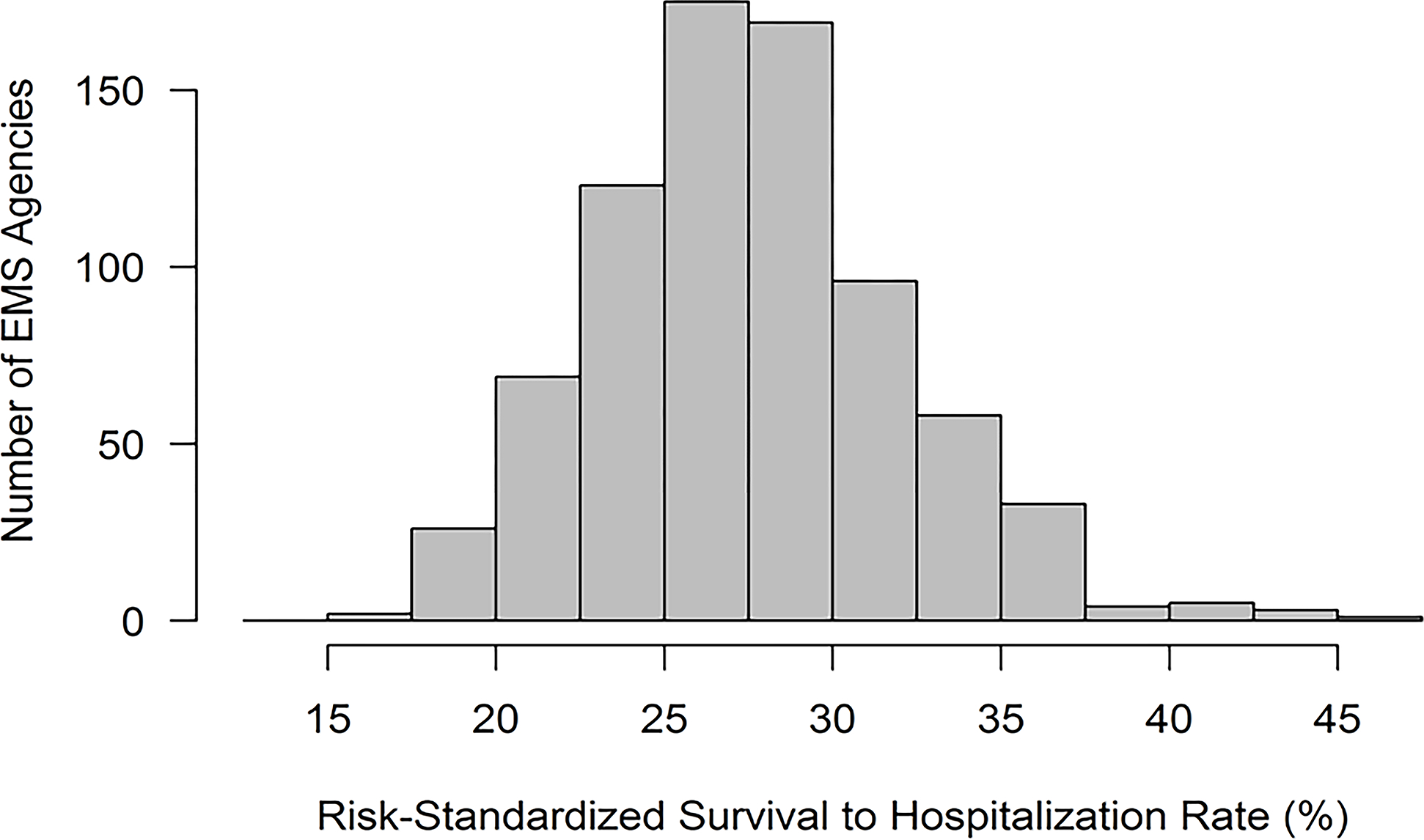
Results: Across 764 EMS agencies comprising 258 342 OHCAs, the median risk-standardized rate of survival to hospital admission was 27.3% (interquartile range, 24.5%-30.1%; range: 16.0%-45.6%). The adjusted median odds ratio was 1.35 (95% CI, 1.32-1.39), denoting that the odds of survival of 2 patients with identical covariates varied by 35% at 2 randomly selected EMS agencies. EMS agencies in the lowest quartile of risk-standardized survival had longer EMS response times when compared with the highest quartile (12.0±3.4 versus 9.0±2.6 minutes; P<0.001), and a higher proportion of OHCAs with termination of resuscitation without meeting futility criteria (27.9±16.1% versus 18.9±11.4%; P<0.001).
Conclusions: Survival after OHCA varies widely across EMS agencies. EMS response times and termination of resuscitation practices were associated with agency-level rates of survival to hospital admission, suggesting potentially modifiable practices which can improve OHCA survival.
Keywords: emergency medical services; geographic locations; out-of-hospital cardiac arrest; resuscitation; survival.
Conflict of interest statement
Figures
References
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, et al. Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association. Circulation. 2019;139:e56–e528. doi: doi: 10.1161/CIR.0000000000000659 - DOI - PubMed
-
- Yan S, Gan Y, Jiang N, Wang R, Chen Y, Luo Z, Zong Q, Chen S, Lv C. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Critical care (London, England). 2020;24:61. doi: 10.1186/s13054-020-2773-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
