

Integrating a Polygenic Risk Score for Coronary Artery Disease as a Risk-Enhancing Factor in the Pooled Cohort Equation: A Cost-Effectiveness Analysis Study
- PMID: 35699184
- PMCID: PMC9238642
- DOI: 10.1161/JAHA.121.025236
Integrating a Polygenic Risk Score for Coronary Artery Disease as a Risk-Enhancing Factor in the Pooled Cohort Equation: A Cost-Effectiveness Analysis Study
Abstract
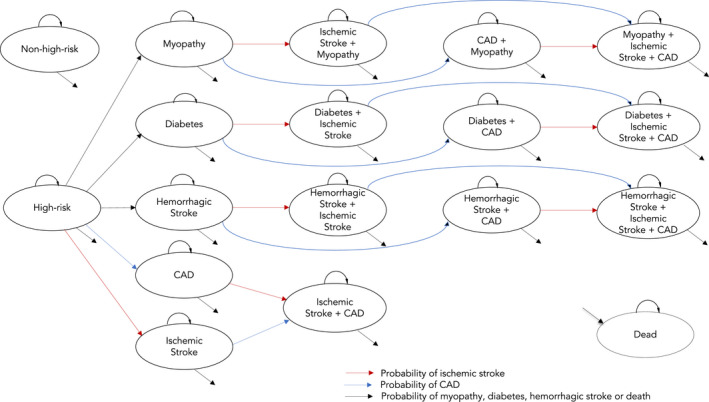
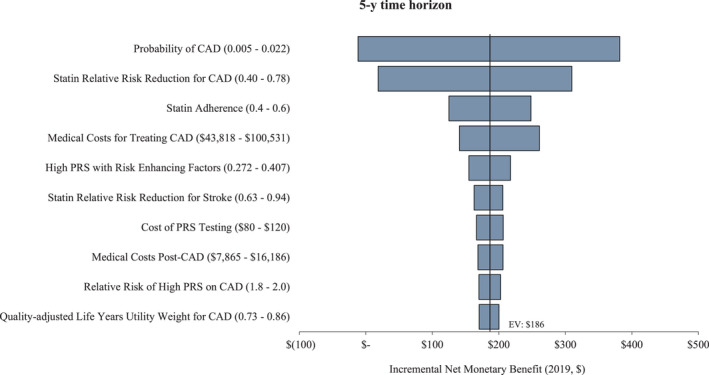
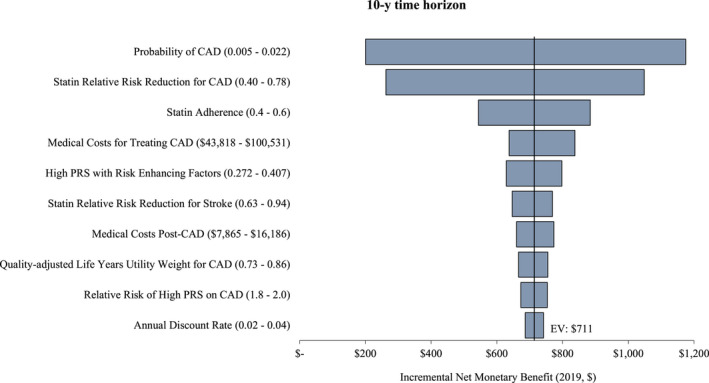
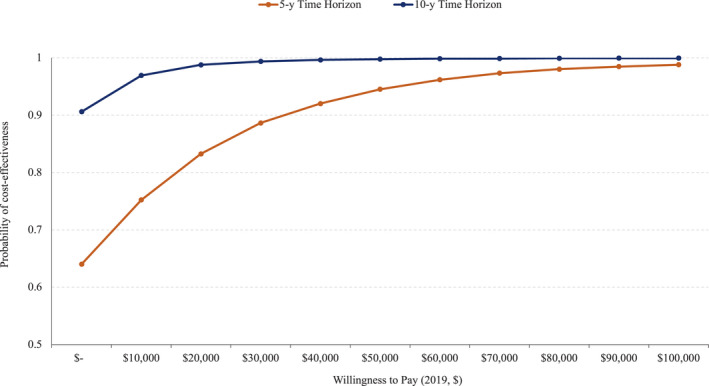
Background Cardiovascular diseases are the leading cause of death in the United States, yet a significant proportion of adults at high risk remain undetected by standard screening practices. Polygenic risk score for coronary artery disease (CAD-PRS) improves precision in determining the 10-year risk of atherosclerotic cardiovascular disease but health benefits and health care costs associated with CAD-PRS are unknown. We examined the cost-effectiveness of including CAD-PRS as a risk-enhancing factor in the pooled cohort equation (PCE)-the standard of care for determining the risk of atherosclerotic cardiovascular disease-versus PCE alone. Methods and Results We applied a Markov model on a cohort of 40-year-old individuals with borderline or intermediate 10-year risk (5% to <20%) for atherosclerotic cardiovascular disease to identify those in the top quintile of the CAD-PRS distribution who are at high risk and eligible for statin prevention therapy. Health outcomes examined included coronary artery disease (CAD; ie, myocardial infarction) and ischemic stroke. The model projected medical costs (2019 US$) of screening for CAD, statin prevention therapy, treatment, and monitoring patients living with CAD or ischemic stroke and quality-adjusted life-years for PCE+CAD-PRS versus PCE alone. Deterministic and probabilistic sensitivity analyses and scenario analyses were performed to examine uncertainty in parameter inputs. PCE+CAD-PRS was dominant compared with PCE alone in the 5- and 10-year time horizons. We found that, respectively, PCE+CAD-PRS had 0.003 and 0.011 higher mean quality-adjusted life-years and $40 and $181 lower mean costs per person screened, with 29 and 50 fewer events of CAD and ischemic stroke in a cohort of 10 000 individuals compared with PCE alone. The risk of developing CAD, the effectiveness of statin prevention therapy, and the cost of treating CAD had the largest impact on the cost per quality-adjusted life-year gained. However, this cost remained below the $50 000 willingness-to-pay threshold except when the annual risk of developing CAD was <0.006 in the 5-year time horizon. Results from Monte Carlo simulation indicated that PCE+CAD-PRS would be cost-effective. with the probability of 94% and 99% at $50 000 willingness-to-pay threshold in the 5- and 10-year time horizon, respectively. Conclusions Implementing CAD-PRS as a risk-enhancing factor in the PCE to determine the risk of atherosclerotic cardiovascular disease reduced the mean cost per individual, improved quality-adjusted life-years, and averted future events of CAD and ischemic stroke when compared with PCE alone.
Keywords: coronary artery disease; cost‐effectiveness; polygenic risk score.
Figures
Similar articles
-
Cost-effectiveness analysis of implementing polygenic risk score in a workplace cardiovascular disease prevention program.Front Public Health. 2023 Jul 11;11:1139496. doi: 10.3389/fpubh.2023.1139496. eCollection 2023. Front Public Health. 2023. PMID: 37497026 Free PMC article.
-
Predictive Utility of a Coronary Artery Disease Polygenic Risk Score in Primary Prevention.JAMA Cardiol. 2023 Feb 1;8(2):130-137. doi: 10.1001/jamacardio.2022.4466. JAMA Cardiol. 2023. PMID: 36576811 Free PMC article.
-
European and US Guideline-Based Statin Eligibility, Genetically Predicted Coronary Artery Disease, and the Risk of Major Coronary Events.J Am Heart Assoc. 2024 May 7;13(9):e032831. doi: 10.1161/JAHA.123.032831. Epub 2024 Apr 19. J Am Heart Assoc. 2024. PMID: 38639378 Free PMC article.
-
Implications of Coronary Artery Calcium Testing for Treatment Decisions Among Statin Candidates According to the ACC/AHA Cholesterol Management Guidelines: A Cost-Effectiveness Analysis.JACC Cardiovasc Imaging. 2017 Aug;10(8):938-952. doi: 10.1016/j.jcmg.2017.04.014. JACC Cardiovasc Imaging. 2017. PMID: 28797417 Review.
-
Screening for Coronary Artery Disease in Cancer Survivors: JACC: CardioOncology State-of-the-Art Review.JACC CardioOncol. 2023 Feb 21;5(1):22-38. doi: 10.1016/j.jaccao.2022.12.007. eCollection 2023 Feb. JACC CardioOncol. 2023. PMID: 36875910 Free PMC article. Review.
Cited by
-
Polygenic Risk Scores: The Next Step for Improved Risk Stratification in Coronary Artery Disease?Arq Bras Cardiol. 2024 Sep;121(9):e20240252. doi: 10.36660/abc.20240252. Arq Bras Cardiol. 2024. PMID: 39352188 Free PMC article. Review. English, Portuguese.
-
Estimating Disorder Probability Based on Polygenic Prediction Using the BPC Approach.medRxiv [Preprint]. 2025 Mar 21:2024.01.12.24301157. doi: 10.1101/2024.01.12.24301157. medRxiv. 2025. PMID: 38260678 Free PMC article. Preprint.
-
Machine learning models for predicting blood pressure phenotypes by combining multiple polygenic risk scores.Sci Rep. 2024 May 30;14(1):12436. doi: 10.1038/s41598-024-62945-9. Sci Rep. 2024. PMID: 38816422 Free PMC article.
-
Implementing Reporting Standards for Polygenic Risk Scores for Atherosclerotic Cardiovascular Disease.Curr Atheroscler Rep. 2023 Jun;25(6):323-330. doi: 10.1007/s11883-023-01104-3. Epub 2023 May 24. Curr Atheroscler Rep. 2023. PMID: 37223852 Free PMC article. Review.
-
Genetics of diabetes.World J Diabetes. 2023 Jun 15;14(6):656-679. doi: 10.4239/wjd.v14.i6.656. World J Diabetes. 2023. PMID: 37383588 Free PMC article. Review.
References
-
- Aragam KG, Dobbyn A, Judy R, Chaffin M, Chaudhary K, Hindy G, Cagan A, Finneran P, Weng LC, Loos RJ, et al. Limitations of contemporary guidelines for managing patients at high genetic risk of coronary artery disease. J Am Coll Cardiol. 2020;75:2769–2780. doi: 10.1016/j.jacc.2020.04.027 - DOI - PMC - PubMed
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, Himmelfarb CD, Khera A, Lloyd‐Jones D, McEvoy JW, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140:e596–e646. doi: 10.1016/j.jacc.2019.03.010 - DOI - PMC - PubMed
-
- Figtree GA, Vernon ST, Hadziosmanovic N, Sundström J, Alfredsson J, Arnott C, Delatour V, Leósdóttir M, Hagström E. Mortality in STEMI patients without standard modifiable risk factors: a sex‐disaggregated analysis of SWEDEHEART registry data. Lancet. 2021;397:1085–1094. doi: 10.1016/S0140-6736(21)00272-5 - DOI - PubMed
-
- Khera AV, Chaffin M, Aragam KG, Haas ME, Roselli C, Choi SH, Natarajan P, Lander ES, Lubitz SA, Ellinor PT, et al. Genome‐wide polygenic scores for common diseases identify individuals with risk equivalent to monogenic mutations. Nat Genet. 2018;50:1219–1224. doi: 10.1038/s41588-018-0183-z - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
