

Efficacy of Cochleated Amphotericin B in Mouse and Human Mucocutaneous Candidiasis
- PMID: 35699443
- PMCID: PMC9295580
- DOI: 10.1128/aac.00308-22
Efficacy of Cochleated Amphotericin B in Mouse and Human Mucocutaneous Candidiasis
Abstract
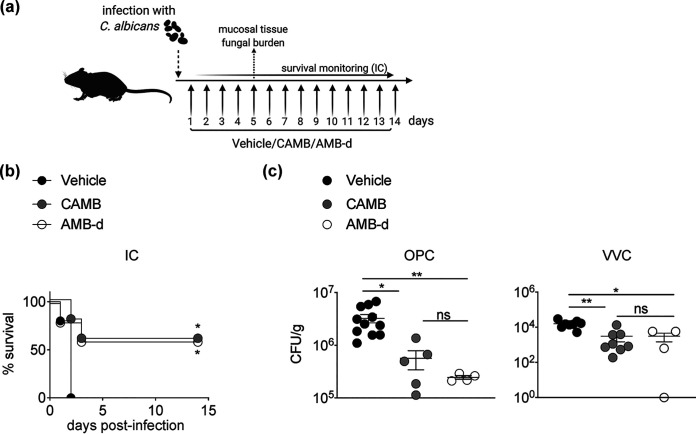
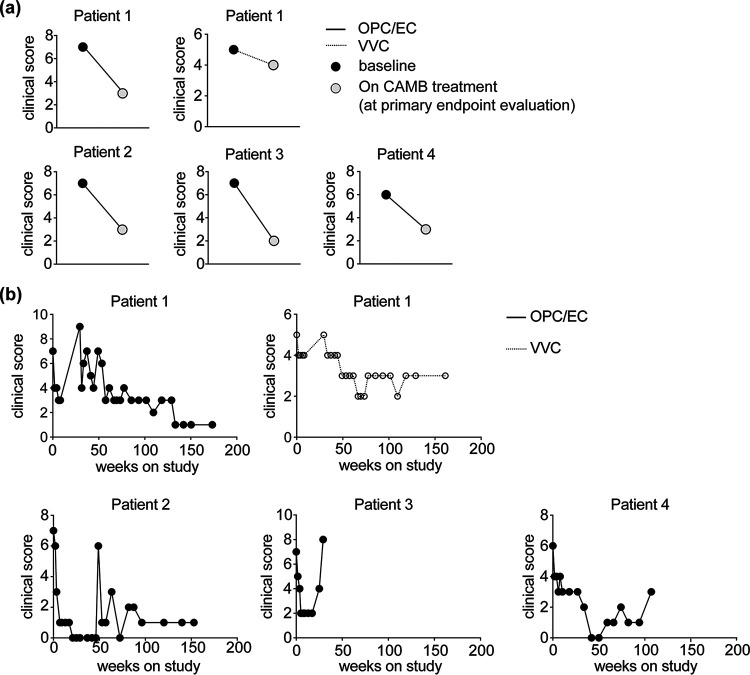
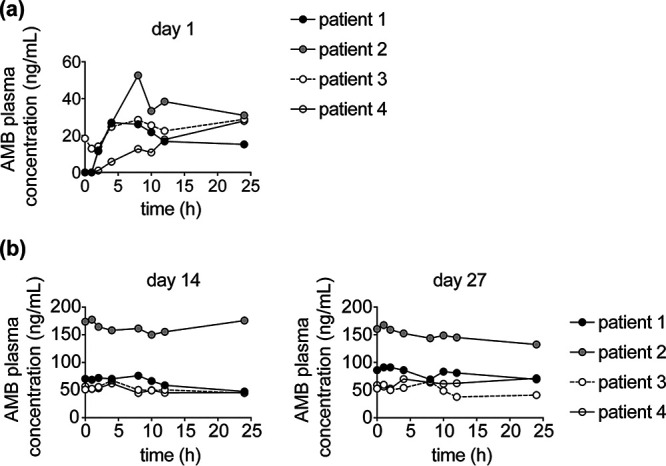
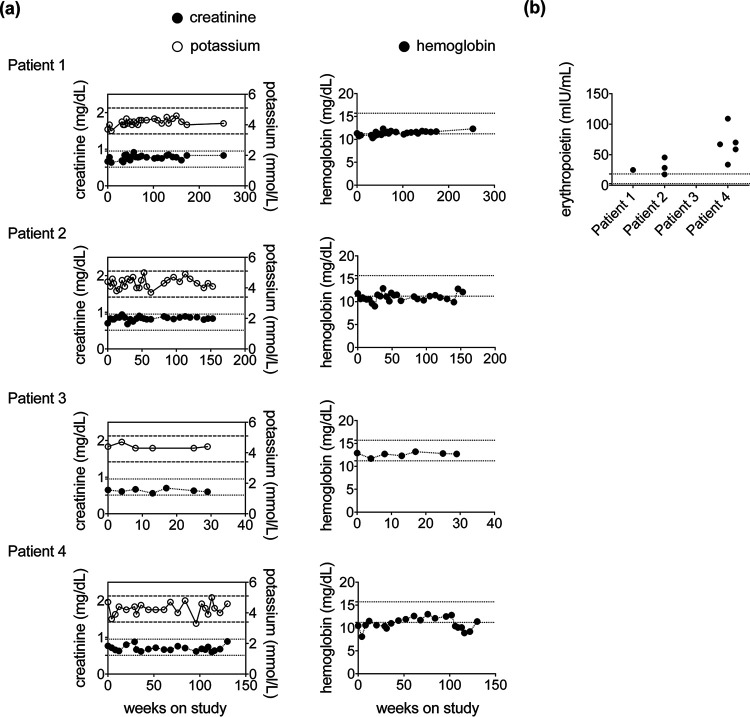
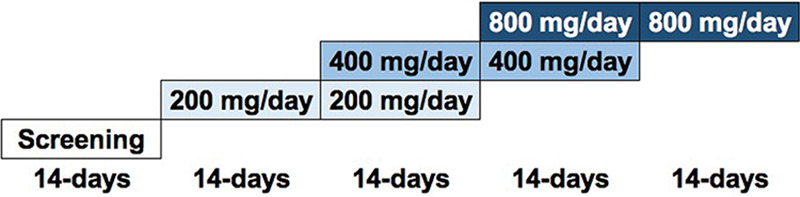
Candida albicans causes debilitating, often azole-resistant, infections in patients with chronic mucocutaneous candidiasis (CMC). Amphotericin B (AMB) resistance is rare, but AMB use is limited by parenteral administration and nephrotoxicity. In this study, we evaluated cochleated AMB (CAMB), a new oral AMB formulation, in mouse models of oropharyngeal candidiasis (OPC) and vulvovaginal candidiasis (VVC) and in patients with azole-resistant CMC. OPC and VVC were modeled in Act1-/- mice, and mucosal tissue fungal burden was assessed after once-daily treatment with CAMB, vehicle, or AMB-deoxycholate (AMB-d). Four patients with azole-resistant CMC enrolled in a phase 2 CAMB dose-escalation study. The primary endpoint was clinical improvement at 2 weeks followed by optional extension for long-term CMC suppression to assess safety and efficacy. CAMB-treated mice had significantly reduced tongue and vaginal fungal burdens compared to vehicle-treated mice and exhibited comparable fungal burden reduction relative to AMB-d-treated mice. All CAMB-treated patients reached clinical efficacy by 2 weeks, three at 400 mg twice daily and one at 200 mg twice-daily dosing. All patients continued to the extension phase, with three having sustained clinical improvement of OPC and esophageal candidiasis (EC) for up to 60 months. One patient had a relapse of esophageal symptoms at week 24 and was withdrawn from further study. Clinical responses were not seen for onychomycosis or VVC. CAMB was safe and well-tolerated, without any evidence of nephrotoxicity. In summary, oral CAMB reduced tongue and vaginal fungal burdens during murine candidiasis. A proof-of-concept clinical trial in human CMC showed efficacy with good tolerability and safety. This study has been registered at ClinicalTrials.gov under identifier NCT02629419.
Keywords: amphotericin B; chronic mucocutaneous candidiasis; cochleated; mouse model; mucosal candidiasis; phase 2 trial.
Conflict of interest statement
The authors declare no conflict of interest.
T.M. and R.M. are employees of Matinas Biopharma Nanotechnologies, Inc., which is the producer of CAMB. M.S.L. and A.F.F. received funding support from Matinas Biopharma for these studies. No other authors have conflicts of interest to declare.
Figures
References
-
- Milner JD, Brenchley JM, Laurence A, Freeman AF, Hill BJ, Elias KM, Kanno Y, Spalding C, Elloumi HZ, Paulson ML, Davis J, Hsu A, Asher AI, O'Shea J, Holland SM, Paul WE, Douek DC. 2008. Impaired T(H)17 cell differentiation in subjects with autosomal dominant hyper-IgE syndrome. Nature 452:773–776. 10.1038/nature06764. - DOI - PMC - PubMed
-
- Puel A, Cypowyj S, Bustamante J, Wright JF, Liu L, Lim HK, Migaud M, Israel L, Chrabieh M, Audry M, Gumbleton M, Toulon A, Bodemer C, El-Baghdadi J, Whitters M, Paradis T, Brooks J, Collins M, Wolfman NM, Al-Muhsen S, Galicchio M, Abel L, Picard C, Casanova J-L. 2011. Chronic mucocutaneous candidiasis in humans with inborn errors of interleukin-17 immunity. Science 332:65–68. 10.1126/science.1200439. - DOI - PMC - PubMed
-
- Ferre EMN, Rose SR, Rosenzweig SD, Burbelo PD, Romito KR, Niemela JE, Rosen LB, Break TJ, Gu W, Hunsberger S, Browne SK, Hsu AP, Rampertaap S, Swamydas M, Collar AL, Kong HH, Lee C-CR, Chascsa D, Simcox T, Pham A, Bondici A, Natarajan M, Monsale J, Kleiner DE, Quezado M, Alevizos I, Moutsopoulos NM, Yockey L, Frein C, Soldatos A, Calvo KR, Adjemian J, Similuk MN, Lang DM, Stone KD, Uzel G, Kopp JB, Bishop RJ, Holland SM, Olivier KN, Fleisher TA, Heller T, Winer KK, Lionakis MS. 2016. Redefined clinical features and diagnostic criteria in autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. JCI Insight 1:e88782. 10.1172/jci.insight.88782. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
