

Strategy for lung parenchyma-sparing bronchial resection: a case series report
- PMID: 35699490
- PMCID: PMC9336563
- DOI: 10.1093/icvts/ivac166
Strategy for lung parenchyma-sparing bronchial resection: a case series report
Abstract
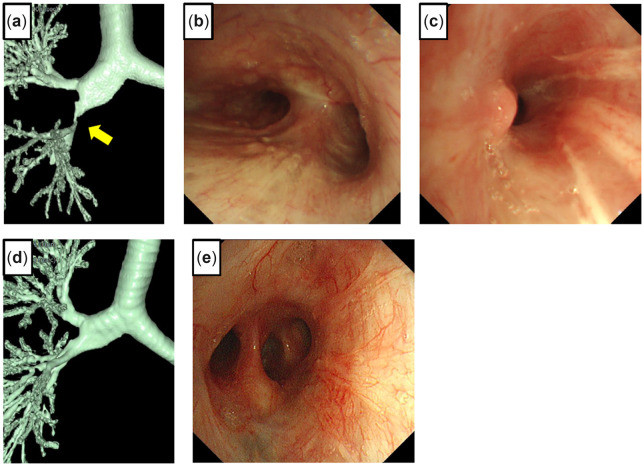
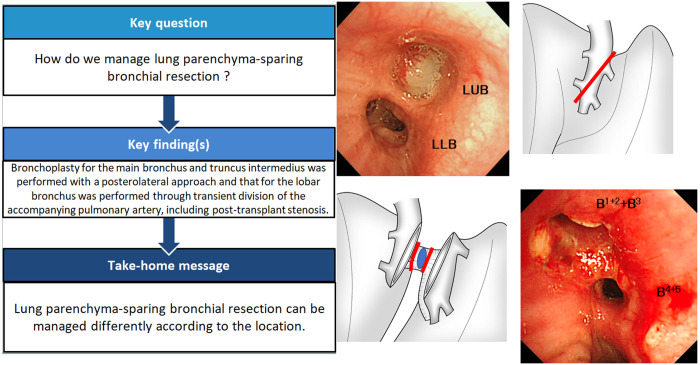
Lung parenchyma-sparing bronchial resection is uncommon, and the operative procedure depends on the cause and location of the stenosis. We present 6 cases and discuss the different surgical strategies for sleeve resection of the central airway without lung resection. Bronchoplasty for the main bronchus and truncus intermedius was performed with a posterolateral approach. We resected the right main bronchus including the right lateral wall of the lower trachea and half of the carina obliquely and performed an anastomosis. The tumour in the left lobar bronchus was exposed and removed by transient division of the accompanying pulmonary artery. Although post-transplant stenosis and malacia can pose a challenge, bronchoplasty can be used as a definitive treatment in experienced centres.
Keywords: Bronchial sleeve resection; Bronchoplasty; Lung cancer; Lung parenchyma-sparing.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures





References
-
- Hamada S, Ohsumi A, Goto T, Hamaji M, Date H, Hirai T.. Delayed right main bronchus stenosis with involvement of the tracheal carina after blunt chest trauma: successful treatment with tracheobronchial anastomosis. Arch Bronconeumol 2020; S0300-2896(20)30341-0.[TQ1] - PubMed
-
- Lucchi M, Melfi F, Ribechini A, Dini P, Duranti L, Fontanini G. et al. Sleeve and wedge parenchyma-sparing bronchial resections in low-grade neoplasms of the bronchial airway. J Thorac Cardiovasc Surg 2007;134:373–7. - PubMed
-
- Stamatis G, Fechner S, Rocha M, Weinreich G.. Resection of the tracheobronchial bifurcation with complete preservation of lung parenchyma. Ann Thorac Surg 2017;104:1741–7. - PubMed
-
- Dell'Amore A, Chen L, Monaci N, Campisi A, Wang Z, Mammana M. et al. Total lung-sparing surgery for tracheobronchial low-grade malignancies. Ann Thorac Surg 2021;112:450–8. - PubMed
-
- Newton JR Jr, Grillo HC, Mathise DJ.. Main bronchial sleeve resection with pulmonary conservation. Ann Thorac Surg 1991;52:1272–80. - PubMed
