

A Population-Based Study of Treatment and Survival in Older Glioma Patients
- PMID: 35699501
- PMCID: PMC8882385
- DOI: 10.1093/jncics/pkac010
A Population-Based Study of Treatment and Survival in Older Glioma Patients
Abstract
Background: Population-based analyses of patterns of care and survival of older patients diagnosed with grade II-III oligodendroglioma (OLI) or astrocytoma (AST) can aid clinicians in their understanding and care of these patients.
Methods: We identified patients diagnosed between 2006 and 2015 with primary glioma diagnoses (OLI or AST) who were older than 65 years using the latest release of the Surveillance, Epidemiology, and End Results-Medicare-linked database. Medicare claims were used to identify cancer treatments (surgery, chemotherapy, and radiation therapy) from 2006 to 2016. Kaplan-Meier methodology was used to describe overall survival (OS). Cox proportional hazards regression was used to associate variables of interest, including treatments in a time-dependent manner, with OS. Hazard ratios (HRs) and 95% confidence intervals (CIs) from multivariable, cause-specific competing risk models identified associations with treatments. All statistical tests were 2-sided.
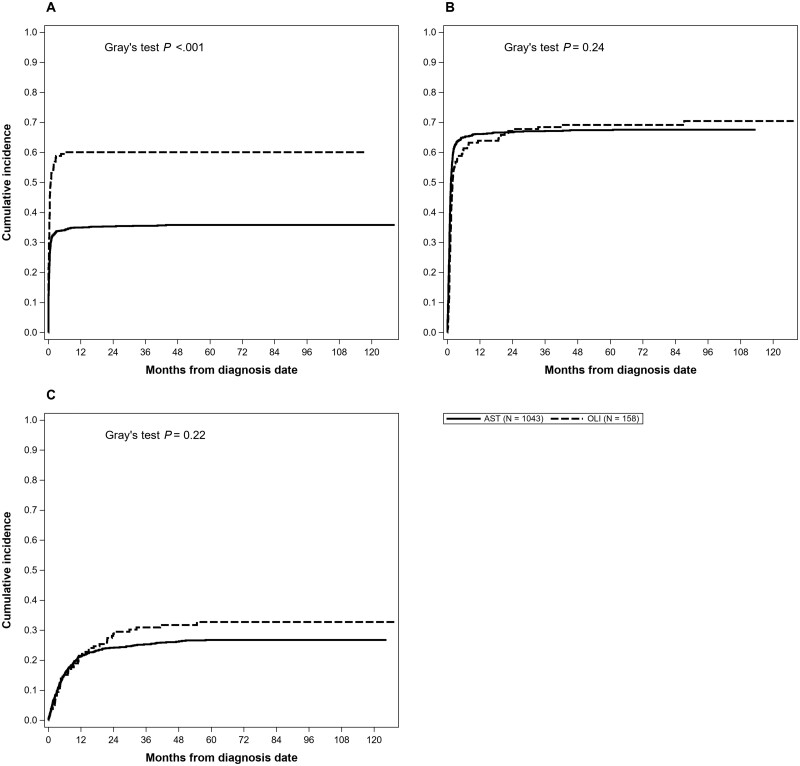
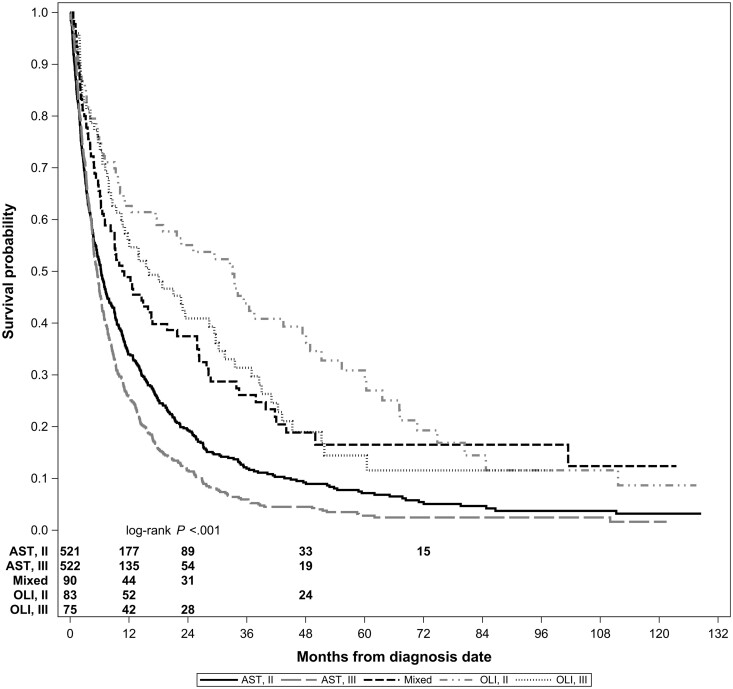
Results: We identified 1291 patients comprising 158 with OLI, 1043 with AST, and 90 with mixed histologies. Median OS was 6.5 (95% CI = 6.1 to 7.3) months for the overall cohort, 22.6 (95% CI = 13.9 to 33.1) months for OLI, and 5.8 (95% CI = 5.3 to 6.4) months for AST. Patients who received surgery and patients who received both chemotherapy and radiation therapy in combination experienced better OS (HR = 0.87, 95% CI = 0.79 to 0.96, and HR = 0.58, 95% CI = 0.35 to 0.96, respectively). Over the time frame studied, there was a 4.0% increase per year in prescription of chemotherapy (P = .03) and a 2.0% improvement in OS for each calendar year (P = .003).
Conclusions: We provide population-based evidence that patients older than 65 years with grade II-III glioma have experienced increased chemotherapy use as well as improvement in survival over time.
© The Author(s) 2022. Published by Oxford University Press.
Figures
References
-
- Davis ME. Epidemiology and overview of gliomas. Semin Oncol Nurs. 2018;34(5):420–429. - PubMed
-
- Miller KD, Ostrom QT, Kruchko C, et al. Brain and other central nervous system tumor statistics, 2021. CA Cancer J Clin. 2021;71(5):381–406. - PubMed
-
- Hutchins LF, Unger JM, Crowley JJ, Coltman CA, Albai KS.. Underrepresentation of patients 65 years of age or older in cancer to treatment trials. N Engl J Med. 1999;341(27):2061–2067. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources