

Validation of Artificial Intelligence Cardiac MRI Measurements: Relationship to Heart Catheterization and Mortality Prediction
- PMID: 35699578
- PMCID: PMC9527336
- DOI: 10.1148/radiol.212929
Validation of Artificial Intelligence Cardiac MRI Measurements: Relationship to Heart Catheterization and Mortality Prediction
Erratum in
-
Validation of Artificial Intelligence Cardiac MRI Measurements: Relationship to Heart Catheterization and Mortality Prediction.Radiology. 2022 Sep;304(3):E56. doi: 10.1148/radiol.229014. Radiology. 2022. PMID: 35994400 Free PMC article. No abstract available.
Abstract
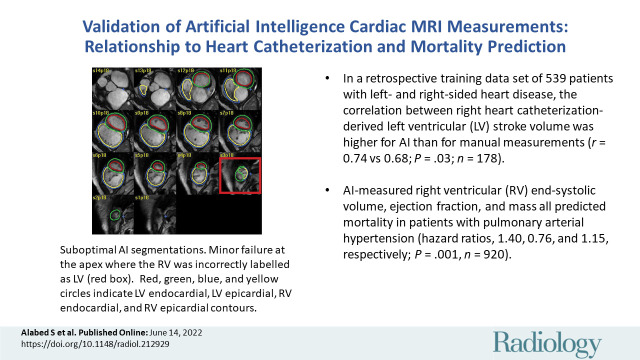
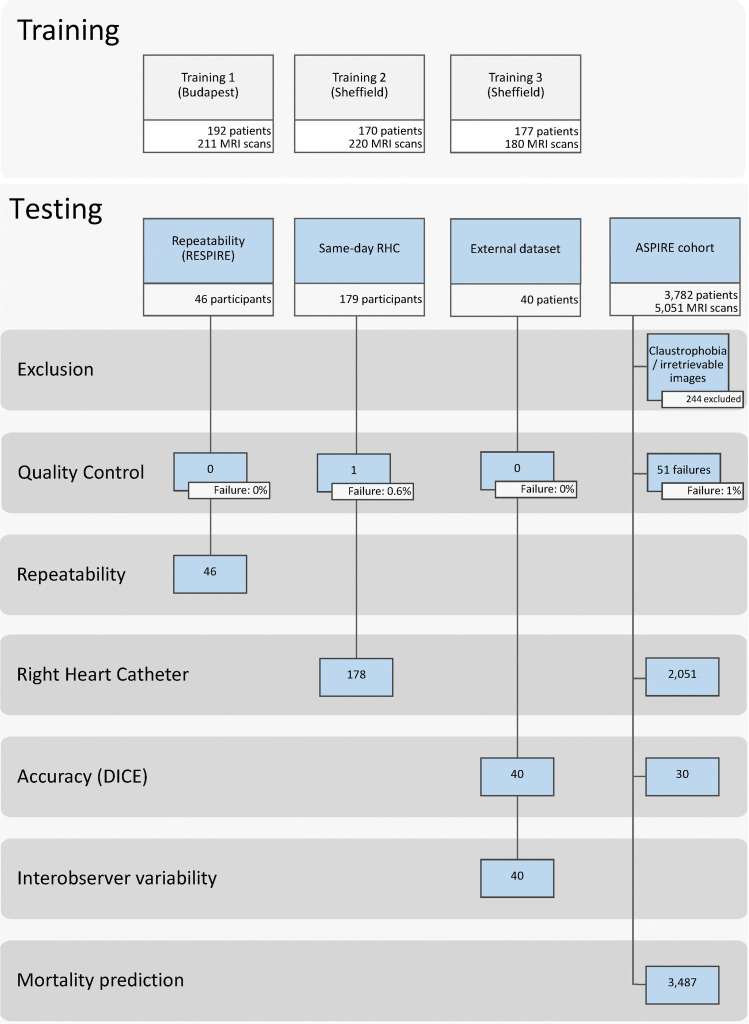
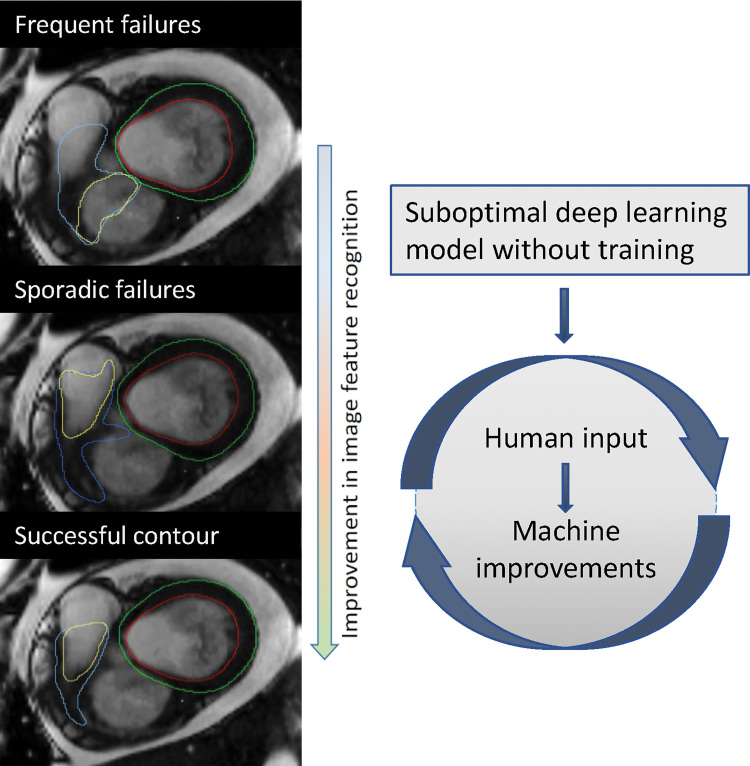
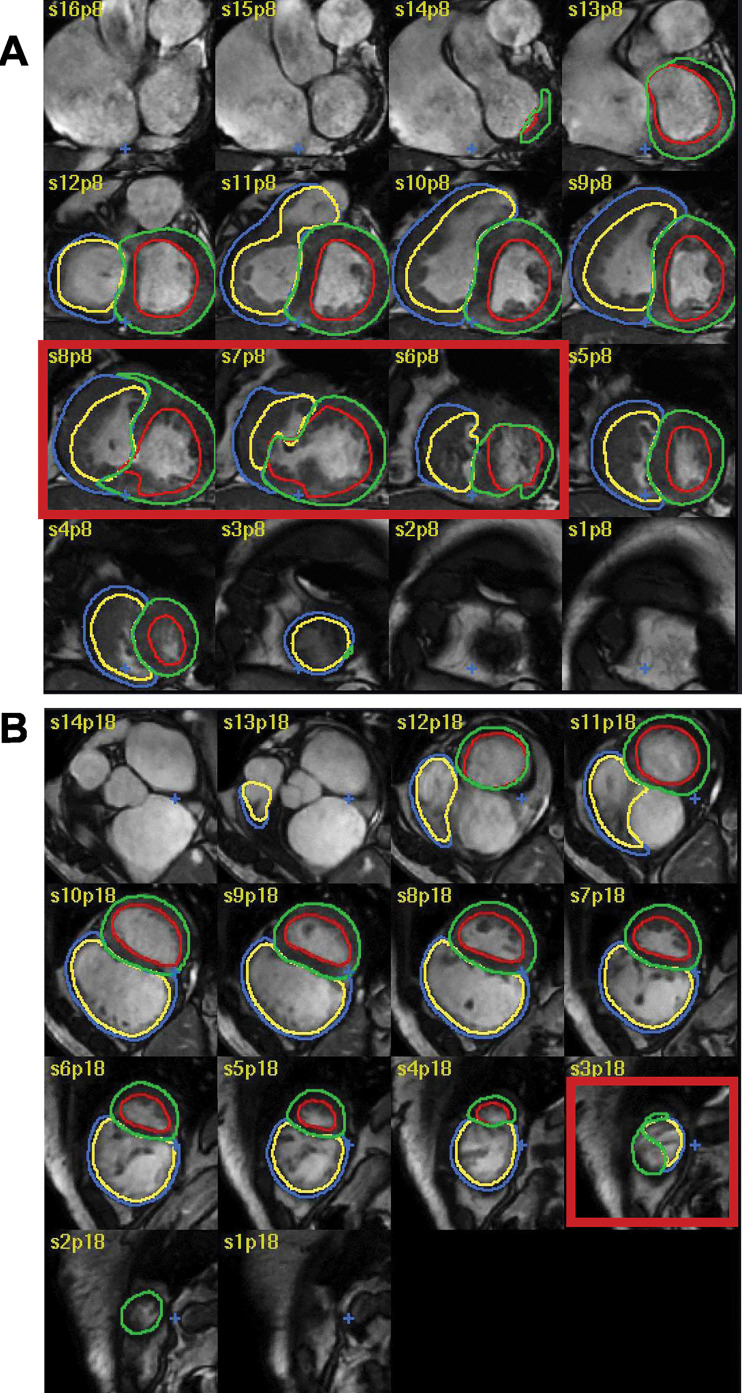
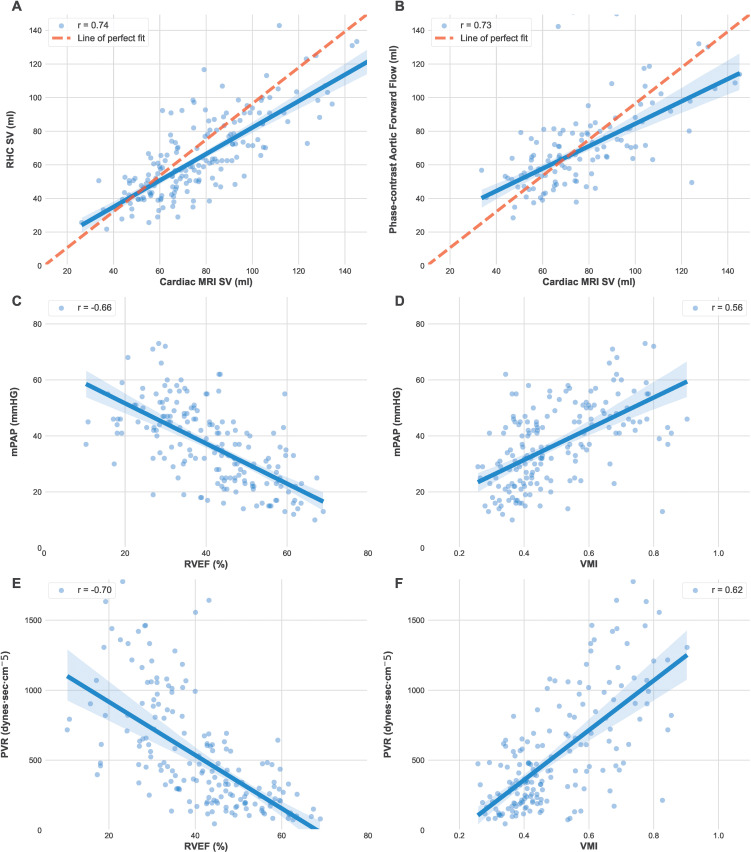
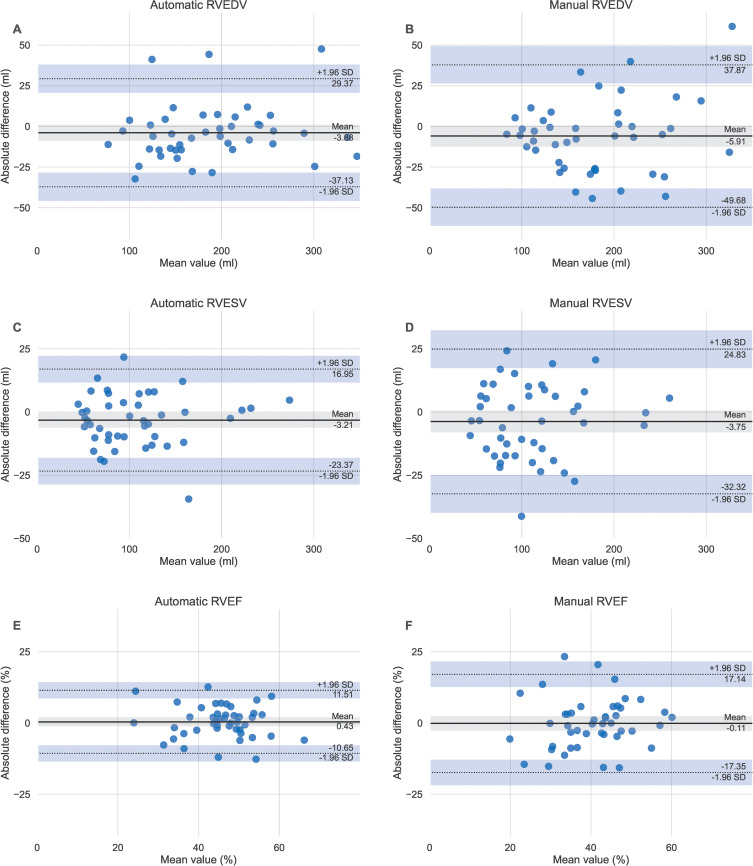
Background Cardiac MRI measurements have diagnostic and prognostic value in the evaluation of cardiopulmonary disease. Artificial intelligence approaches to automate cardiac MRI segmentation are emerging but require clinical testing. Purpose To develop and evaluate a deep learning tool for quantitative evaluation of cardiac MRI functional studies and assess its use for prognosis in patients suspected of having pulmonary hypertension. Materials and Methods A retrospective multicenter and multivendor data set was used to develop a deep learning-based cardiac MRI contouring model using a cohort of patients suspected of having cardiopulmonary disease from multiple pathologic causes. Correlation with same-day right heart catheterization (RHC) and scan-rescan repeatability was assessed in prospectively recruited participants. Prognostic impact was assessed using Cox proportional hazard regression analysis of 3487 patients from the ASPIRE (Assessing the Severity of Pulmonary Hypertension In a Pulmonary Hypertension Referral Centre) registry, including a subset of 920 patients with pulmonary arterial hypertension. The generalizability of the automatic assessment was evaluated in 40 multivendor studies from 32 centers. Results The training data set included 539 patients (mean age, 54 years ± 20 [SD]; 315 women). Automatic cardiac MRI measurements were better correlated with RHC parameters than were manual measurements, including left ventricular stroke volume (r = 0.72 vs 0.68; P = .03). Interstudy repeatability of cardiac MRI measurements was high for all automatic measurements (intraclass correlation coefficient range, 0.79-0.99) and similarly repeatable to manual measurements (all paired t test P > .05). Automated right ventricle and left ventricle cardiac MRI measurements were associated with mortality in patients suspected of having pulmonary hypertension. Conclusion An automatic cardiac MRI measurement approach was developed and tested in a large cohort of patients, including a broad spectrum of right ventricular and left ventricular conditions, with internal and external testing. Fully automatic cardiac MRI assessment correlated strongly with invasive hemodynamics, had prognostic value, were highly repeatable, and showed excellent generalizability. Clinical trial registration no. NCT03841344 Published under a CC BY 4.0 license. Online supplemental material is available for this article. See also the editorial by Ambale-Venkatesh and Lima in this issue. An earlier incorrect version appeared online. This article was corrected on June 27, 2022.
Conflict of interest statement
Figures
Comment in
-
Human-in-the-Loop Artificial Intelligence in Cardiac MRI.Radiology. 2022 Oct;305(1):80-81. doi: 10.1148/radiol.221132. Epub 2022 Jun 14. Radiology. 2022. PMID: 35699584 No abstract available.
References
-
- Tao Q, Yan W, Wang Y, et al. . Deep Learning-based Method for Fully Automatic Quantification of Left Ventricle Function from Cine MR Images: A Multivendor, Multicenter Study. Radiology 2019;290(1):81–88. - PubMed
-
- Petitjean C, Zuluaga MA, Bai W, et al. . Right ventricle segmentation from cardiac MRI: a collation study. Med Image Anal 2015;19(1):187–202. - PubMed
-
- Kiely DG, Elliot CA, Sabroe I, Condliffe R. Pulmonary hypertension: diagnosis and management. BMJ 2013;346:f2028. - PubMed
-
- Hurdman J, Condliffe R, Elliot CA, et al. . ASPIRE registry: assessing the Spectrum of Pulmonary hypertension Identified at a REferral centre. Eur Respir J 2012;39(4):945–955. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
