

Design of the COmbinatioN effect of FInerenone anD EmpaglifloziN in participants with chronic kidney disease and type 2 diabetes using a UACR Endpoint study (CONFIDENCE)
- PMID: 35700142
- PMCID: PMC10064838
- DOI: 10.1093/ndt/gfac198
Design of the COmbinatioN effect of FInerenone anD EmpaglifloziN in participants with chronic kidney disease and type 2 diabetes using a UACR Endpoint study (CONFIDENCE)
Abstract
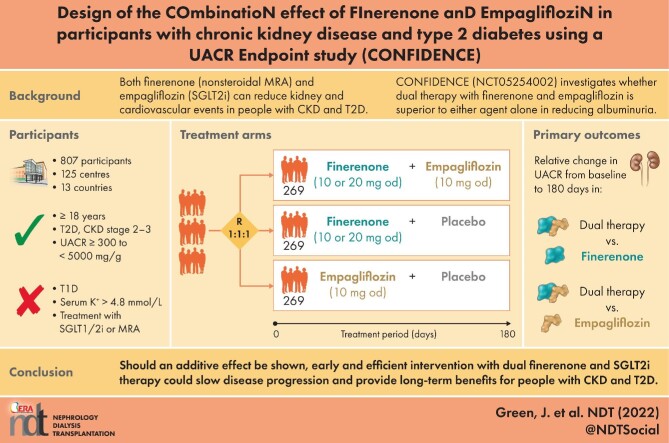
Background: Despite available interventions, people with type 2 diabetes (T2D) remain at risk of chronic kidney disease (CKD). Finerenone, a potent and selective nonsteroidal mineralocorticoid receptor antagonist, and sodium-glucose cotransporter 2 inhibitors (SGLT2is) can reduce both kidney and cardiovascular risks in people with CKD and T2D. Here we outline the design of a study to investigate whether dual therapy with finerenone and an SGLT2i is superior to either agent alone.
Methods: CONFIDENCE (NCT05254002) is a randomized, controlled, double-blind, double-dummy, international, multicenter, three-armed, parallel-group, 7.5 - to 8.5-month, Phase 2 study in 807 adults with T2D, stage 2-3 CKD and a urine albumin:creatinine ratio (UACR) ≥300-<5000 mg/g. The primary objective is to demonstrate that 6 months of dual therapy comprising finerenone and the SGLT2i empagliflozin is superior for reducing albuminuria versus either agent alone. Interventions will be once-daily finerenone 10 mg or 20 mg (target dose) plus empagliflozin 10 mg, or empagliflozin 10 mg alone, or finerenone 10 mg or 20 mg (target dose) alone.
Results: The primary outcome is a relative change from baseline in UACR among the three groups. Secondary outcomes will further characterize efficacy and safety, including changes in estimated glomerular filtration rate and incident hyperkalemia.
Conclusions: CONFIDENCE is evaluating the safety, tolerability and efficacy of dual use of finerenone and an SGLT2i in adults with CKD and T2D. Should an additive effect be shown, early and efficient intervention with dual finerenone and SGLT2i therapy could slow disease progression and provide long-term benefits for people with CKD and T2D.
Keywords: chronic kidney disease; diabetes; empagliflozin; finerenone; macroalbuminuria.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
The authors wrote the article with the assistance of a medical writer funded by the sponsor. The sponsor was involved in the study design and the writing of the report. J.B.G. has received grant support from Boehringer Ingelheim/Lilly, Merck, Roche and Sanofi/Lexicon and has been a consultant for Boehringer Ingelheim/Lilly, Bayer, AstraZeneca, Sanofi/Lexicon, Hawthorne Effect/Omada, Pfizer and NovoNordisk within the past 3 years. A.K.M. received research funding paid to her employer from Duke Clinical Research Institute, Pfizer, Aurinia, Alexion, Bayer and Calliditas and has received consultancy fees from Bayer, speaker fees from The Primary Care Consortium and royalties from UpToDate. G.B. reports receiving research funding from Bayer, Novo Nordisk and Vascular Dynamics, paid to the University of Chicago Miedicine; acting as a consultant and receiving personal fees from Alnylam, Merck and Relypsa; serving as an editor for the
Figures


References
-
- Kidney Disease: Improving Global Outcomes Diabetes Work Group . KDIGO 2020 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int 2020; 98(4 Suppl): S1–S115 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
