

Prognostic value of left ventricular apical four-chamber longitudinal strain after heart valve surgery in real-world practice
- PMID: 35700980
- PMCID: PMC9539422
- DOI: 10.4097/kja.22201
Prognostic value of left ventricular apical four-chamber longitudinal strain after heart valve surgery in real-world practice
Abstract
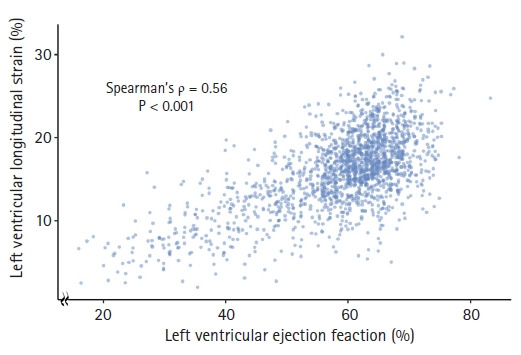
Background: Left ventricular longitudinal strain is an emerging marker of ventricular systolic function. However, the prognostic value of apical four-chamber longitudinal strain after heart valve surgery in real-world clinical practice is uncertain. The authors investigated whether left ventricular apical four-chamber longitudinal strain measured in real-world practice is helpful for predicting postoperative outcomes in patients undergoing heart valve surgery.
Methods: This observational cohort study was conducted in patients who underwent heart valve surgery between January 2014 and December 2018 at a tertiary hospital in South Korea. The exposure of interest was preoperative left ventricular apical four-chamber longitudinal strain. The primary outcome was postoperative all-cause mortality.
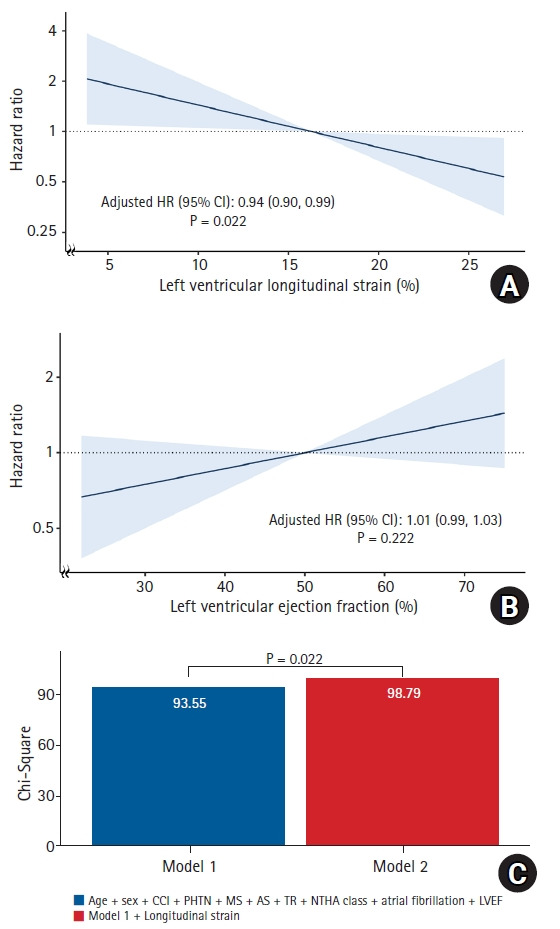
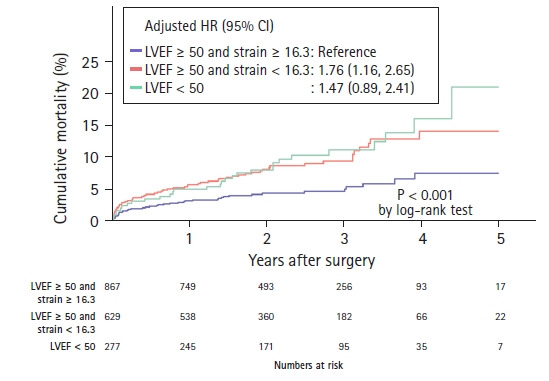
Results: Among 1,773 study patients (median age, 63 years; female, 45.9%), 132 (7.4%) died during a median follow-up of 27.2 months. Preoperative left ventricular apical four-chamber longitudinal strain was significantly associated with all-cause mortality (adjusted hazard ratio, 0.94 per 1% increment in absolute value; 95% CI [0.90, 0.99], P = 0.022), whereas left ventricular ejection fraction (LVEF) was not significantly associated with all-cause mortality (adjusted hazard ratio: 1.01, 95% CI [0.99, 1.03], P = 0.222). Moreover, combining left ventricular apical four-chamber longitudinal strain to the LVEF and conventional prognostic factors enhance the prognostic model for all-cause mortality (P = 0.022).
Conclusions: In patients undergoing heart valve surgery without coronary artery disease, left ventricular apical four-chamber longitudinal strain measured in real-world clinical practice was independently associated with postoperative survival. Left ventricular longitudinal strain measurement may be helpful for outcome prediction after valve surgery.
Keywords: Cardiac surgery; Echocardiography; Heart valve diseases; Morbidity; Mortality; Strain..
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Association between Left Ventricular Longitudinal Strain (GLS) and Prognosis of the Patients Undergoing Heart Valve Surgery with Preserved Left Ventricular Ejection Fraction.Heart Surg Forum. 2023 Dec 26;26(6):E770-E779. doi: 10.59958/hsf.5921. Heart Surg Forum. 2023. PMID: 38178357
-
Long-Term Outcomes After Aortic Valve Surgery in Patients With Asymptomatic Chronic Aortic Regurgitation and Preserved LVEF: Impact of Baseline and Follow-Up Global Longitudinal Strain.JACC Cardiovasc Imaging. 2020 Jan;13(1 Pt 1):12-21. doi: 10.1016/j.jcmg.2018.12.021. Epub 2019 Feb 13. JACC Cardiovasc Imaging. 2020. PMID: 30772216
-
Incremental Prognostic Utility of Left Ventricular Global Longitudinal Strain in Asymptomatic Patients With Significant Chronic Aortic Regurgitation and Preserved Left Ventricular Ejection Fraction.JACC Cardiovasc Imaging. 2018 May;11(5):673-682. doi: 10.1016/j.jcmg.2017.02.016. Epub 2017 Jun 14. JACC Cardiovasc Imaging. 2018. PMID: 28624411
-
Prognostic Value of Left Ventricular Global Longitudinal Strain for Major Adverse Cardiovascular Events in Patients with Aortic Valve Disease: A Meta-Analysis.Cardiology. 2024;149(3):277-285. doi: 10.1159/000536331. Epub 2024 Feb 1. Cardiology. 2024. PMID: 38301616
-
Distribution and Prognostic Significance of Left Ventricular Global Longitudinal Strain in Asymptomatic Significant Aortic Stenosis: An Individual Participant Data Meta-Analysis.JACC Cardiovasc Imaging. 2019 Jan;12(1):84-92. doi: 10.1016/j.jcmg.2018.11.005. JACC Cardiovasc Imaging. 2019. PMID: 30621997
Cited by
-
Application of a new modality for assessing left ventricular function: can strain replace ejection fraction?Korean J Anesthesiol. 2022 Oct;75(5):361-362. doi: 10.4097/kja.22540. Epub 2022 Sep 21. Korean J Anesthesiol. 2022. PMID: 36128641 Free PMC article. No abstract available.
-
Relationship between Preoperative Echocardiographic Parameters and the Incidence of Postoperative Complications in Patients Undergoing Clipping of Unruptured Intracranial Aneurysms: A Retrospective Cohort Study.Medicina (Kaunas). 2023 Sep 22;59(10):1697. doi: 10.3390/medicina59101697. Medicina (Kaunas). 2023. PMID: 37893414 Free PMC article.
-
Percutaneous versus surgical closure of paravalvular leaks in prosthetic valves: A cross-sectional comparison of clinical outcomes.Health Sci Rep. 2024 Aug 23;7(8):e70001. doi: 10.1002/hsr2.70001. eCollection 2024 Aug. Health Sci Rep. 2024. PMID: 39184853 Free PMC article.
References
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Guyton RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:e57–185. - PubMed
-
- Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38:2739–91. - PubMed
-
- Shahian DM, Jacobs JP, Badhwar V, Kurlansky PA, Furnary AP, Cleveland JC, Jr, et al. The Society of Thoracic Surgeons 2018 Adult Cardiac Surgery Risk Models: part 1-background, design considerations, and model development. Ann Thorac Surg. 2018;105:1411–8. - PubMed
-
- Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR, et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41:734–44. - PubMed
-
- Park JJ, Park JB, Park JH, Cho GY. Global longitudinal strain to predict mortality in patients with acute heart failure. J Am Coll Cardiol. 2018;71:1947–57. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
