

Expert clinical pharmacological advice may make an antimicrobial TDM program for emerging candidates more clinically useful in tailoring therapy of critically ill patients
- PMID: 35701812
- PMCID: PMC9199203
- DOI: 10.1186/s13054-022-04050-9
Expert clinical pharmacological advice may make an antimicrobial TDM program for emerging candidates more clinically useful in tailoring therapy of critically ill patients
Abstract
Background: Therapeutic drug monitoring (TDM) may represent an invaluable tool for optimizing antimicrobial therapy in septic patients, but extensive use is burdened by barriers. The aim of this study was to assess the impact of a newly established expert clinical pharmacological advice (ECPA) program in improving the clinical usefulness of an already existing TDM program for emerging candidates in tailoring antimicrobial therapy among critically ill patients.
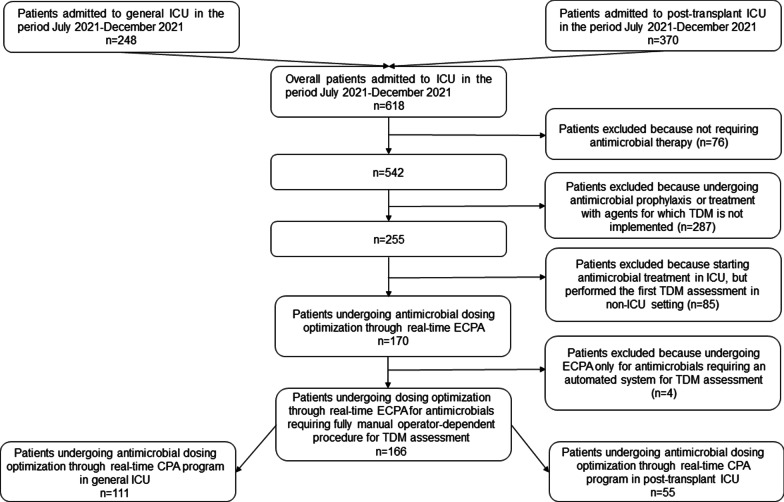
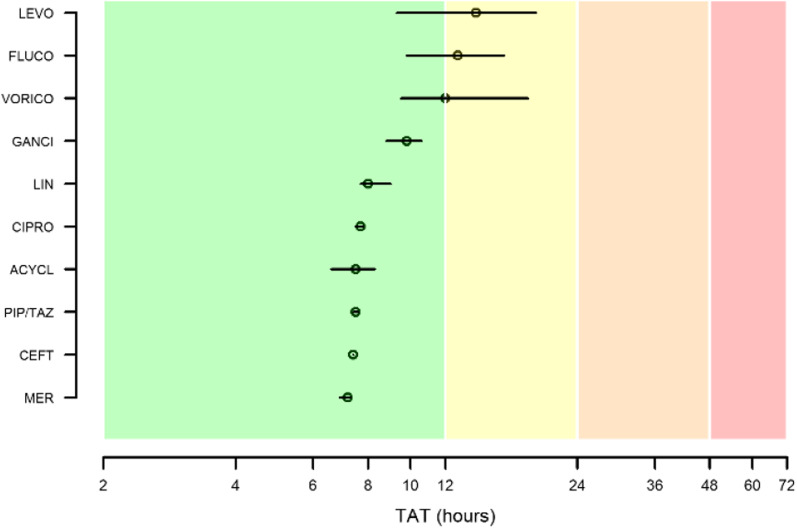
Methods: This retrospective observational study included an organizational phase (OP) and an assessment phase (AP). During the OP (January-June 2021), specific actions were organized by MD clinical pharmacologists together with bioanalytical experts, clinical engineers, and ICU clinicians. During the AP (July-December 2021), the impact of these actions in optimizing antimicrobial treatment of the critically ill patients was assessed. Four indicators of performance of the TDM-guided real-time ECPA program were identified [total TDM-guided ECPAs July-December 2021/total TDM results July-December 2020; total ECPA dosing adjustments/total delivered ECPAs both at first assessment and overall; and turnaround time (TAT) of ECPAs, defined as optimal (< 12 h), quasi-optimal (12-24 h), acceptable (24-48 h), suboptimal (> 48 h)].
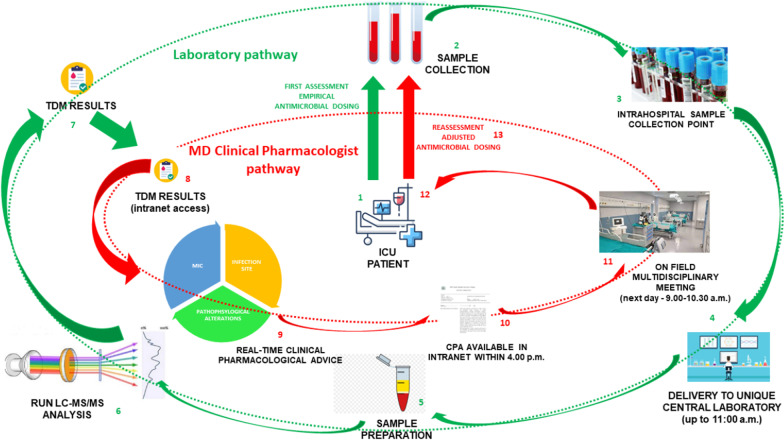
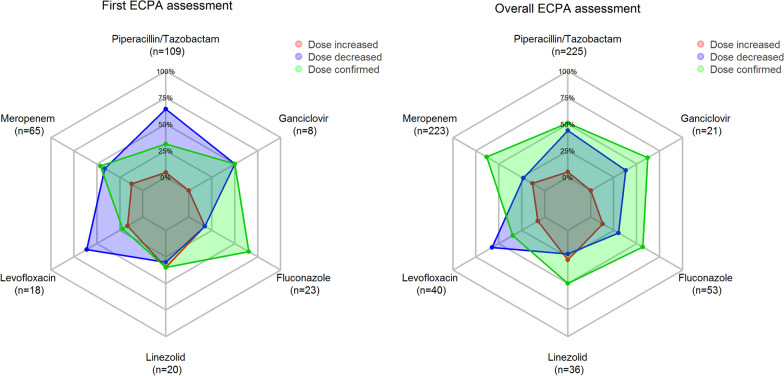
Results: The OP allowed to implement new organizational procedures, to create a dedicated pathway in the intranet system, to offer educational webinars on clinical pharmacology of antimicrobials, and to establish a multidisciplinary team at the morning bedside ICU meeting. In the AP, a total of 640 ECPAs were provided for optimizing 261 courses of antimicrobial therapy in 166 critically ill patients. ECPAs concerned mainly piperacillin-tazobactam (41.8%) and meropenem (24.9%), and also other antimicrobials had ≥ 10 ECPAs (ceftazidime, ciprofloxacin, fluconazole, ganciclovir, levofloxacin, and linezolid). Overall, the pre-post-increase in TDM activity was of 13.3-fold. TDM-guided dosing adjustments were recommended at first assessment in 61.7% of ECPAs (10.7% increases and 51.0% decreases), and overall in 45.0% of ECPAs (10.0% increases and 35.0% decreases). The overall median TAT was optimal (7.7 h) and that of each single agent was always optimal or quasi-optimal.
Conclusions: Multidisciplinary approach and timely expert interpretation of TDM results by MD Clinical Pharmacologists could represent cornerstones in improving the cost-effectiveness of an antimicrobial TDM program for emerging TDM candidates.
Keywords: Critically ill patients; Dosing adjustments; Expert clinical pharmacological advice program; General ICU; Personalized antimicrobial therapy; Transplant ICU; Turnaround time.
© 2022. The Author(s).
Conflict of interest statement
MG reports grants from Angelini S.p.A., outside the submitted work. F.P. reports personal fees from Angelini, Basilea Pharmaceutica, Gilead, Hikma, MSD, Pfizer, Sanofi-Aventis, Shionogi, Thermo Fisher, and Accelerate Diagnostics, outside the submitted work; has participated in speaker’s bureau for Accelerate Diagnostics, Angelini, Basilea Pharmaceutica, Gilead, Hikma, MSD, Pfizer, Sanofi-Aventis, Shionogi, Thermo Fisher, and as consultant for Angelini, Basilea Pharmaceutica, Gilead, MSD, Pfizer, Shionogi, outside the submitted work. P.V. has served as a consultant for bioMérieux, Gilead, Merck Sharp & Dohme, Nabriva, Nordic Pharma, Pfizer, Thermo-Fisher, and Venatorx, and received payment for serving on the speaker’s bureaus for Correvio, Gilead, Merck Sharp & Dohme, Nordic Pharma, and Pfizer, outside the submitted work. The other authors report no potential conflicts of interest for this work.
Figures

References
-
- Roberts JA, Joynt GM, Choi GYS, Gomersall CD, Lipman J. How to optimise antimicrobial prescriptions in the intensive care unit: principles of individualised dosing using pharmacokinetics and pharmacodynamics. Int J Antimicrob Agents. 2012;39:187–192. doi: 10.1016/j.ijantimicag.2011.11.002. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
