

Economic burden of antibiotic-not-susceptible isolates in uncomplicated urinary tract infection: Analysis of a US integrated delivery network database
- PMID: 35701853
- PMCID: PMC9195273
- DOI: 10.1186/s13756-022-01121-y
Economic burden of antibiotic-not-susceptible isolates in uncomplicated urinary tract infection: Analysis of a US integrated delivery network database
Abstract
Background: Uncomplicated urinary tract infections (uUTIs) are one of the most common bacterial infections in the United States (US). Contemporary data are important for understanding the health economic impact of antimicrobial-resistant uUTIs. We compared the economic burden among patients with uUTI isolates susceptible or not-susceptible to the initial antibiotic prescription.
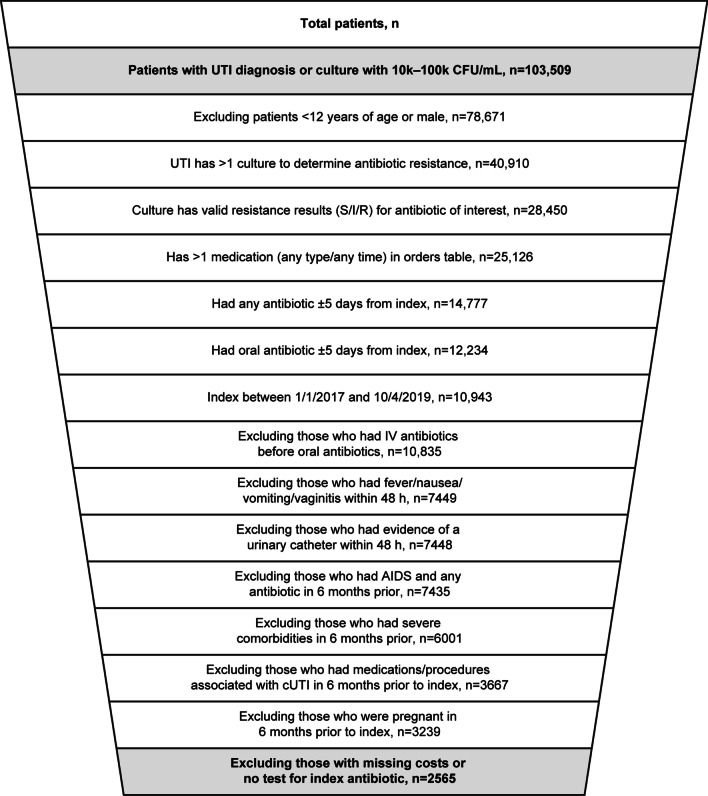
Methods: This retrospective cohort study utilized electronic health record data (1 July 2016-31 March 2020) from a large Mid-Atlantic US integrated delivery network database. Patients were females aged ≥ 12 years with a uUTI, who received oral antibiotic treatment and had ≥ 1 urine culture within ± 5 days of diagnosis. The primary outcome was the difference in healthcare resource use and costs (all-cause, urinary tract infection [UTI]-related) among patients with susceptible versus not-susceptible isolates during the 6 months after the index uUTI diagnosis. Secondary outcomes included: pharmacy costs, hospital admissions and emergency department visits, as well as the probability of uUTI progressing to complicated UTI (cUTI) between patients with susceptible and not-susceptible isolates. Patient outcomes were compared using 1:1 propensity score matching. Winsorized costs were adjusted to 2020 quarter 1 US dollars ($).
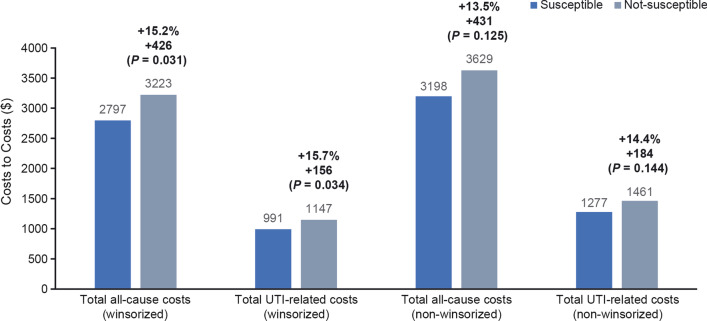
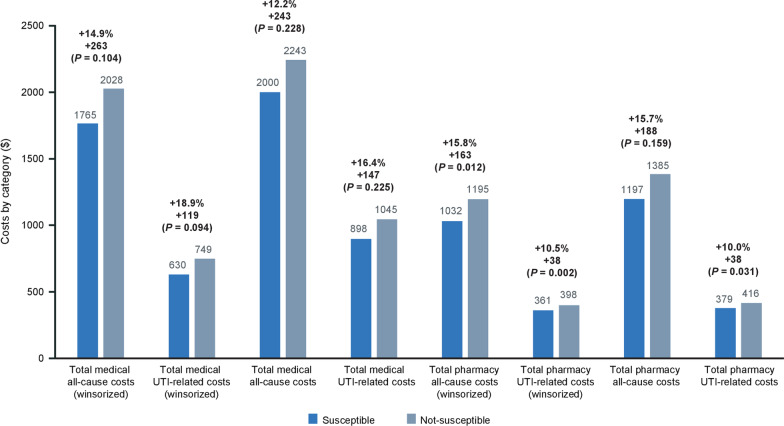
Results: A total of 2565 patients were eligible for analysis. The propensity score-matched sample comprised 2018 patients, with an average age of 44.0 and 41.0 years for the susceptible and not-susceptible populations, respectively. In the 6 months post-index uUTI event, patients with not-susceptible isolates had significantly more all-cause prescriptions orders (+ 1.41 [P = 0.001]), UTI-related prescriptions orders (+ 0.26 [P < 0.001]) and a higher probability of all-cause inpatient (+ 1.4% [P = 0.009]), outpatient (+ 6.1% [P = 0.006]), or UTI-related outpatient (+ 3.7% [P = 0.039]) encounters. Patients with a uUTI and an antibiotic-not-susceptible isolate were significantly more likely to progress to cUTI than those with susceptible isolates (odds ratio: 2.35 [confidence interval: 1.66-3.33; P < 0.001]). Over 6 months, patients with not-susceptible versus susceptible isolates had significantly higher all-cause costs (+ $426 [P = 0.031]) and UTI-related costs (+ $157 [P = 0.034]).
Conclusions: Patients with a uUTI caused by antibiotic-not-susceptible isolates had higher healthcare resource usage, costs, and increased likelihood of progressing to cUTI than those with antibiotic-susceptible isolates.
Keywords: Antibiotic resistance; Costs; Healthcare resource use; Urinary tract infection.
© 2022. The Author(s).
Conflict of interest statement
JS is a former employee of Precision Medicine Group, which received funding from GlaxoSmithKline plc. to conduct this study. AM is an employee of and shareholder in GlaxoSmithKline plc. AVJ is an employee of and shareholder in GlaxoSmithKline plc. FSM-G is an employee of and shareholder in GlaxoSmithKline plc. KE is an employee of Precision Medicine Group, which received funding from GlaxoSmithKline plc. to conduct this study. RT is an employee of Precision Medicine Group, which received funding from GlaxoSmithKline plc. to conduct this study. PR is a former employee of Precision Medicine Group, which received funding from GlaxoSmithKline plc. to conduct this study. MG is a contractor for MedStar Health and received funding from GlaxoSmithKline plc. through Precision Medicine Group to conduct this study. MER is an employee of MedStar Health and received funding from GlaxoSmithKline plc. through Precision Medicine Group to conduct this study.
Figures



References
-
- Gupta K, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011;52(5):e103–e120. doi: 10.1093/cid/ciq257. - DOI - PubMed
-
- Centers for Disease Control Antibiotic Resistance Threats in the United States, 2019 Atlanta, GA: U.S. Department of Health and Human Services, CDC; 2019. 2019.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
