

Silent cerebral infarcts in patients with atrial fibrillation: Clinical implications of an imaging-adjusted CHA2DS2-VASc score
- PMID: 35703042
- PMCID: PMC9550332
- DOI: 10.5603/CJ.a2022.0055
Silent cerebral infarcts in patients with atrial fibrillation: Clinical implications of an imaging-adjusted CHA2DS2-VASc score
Abstract
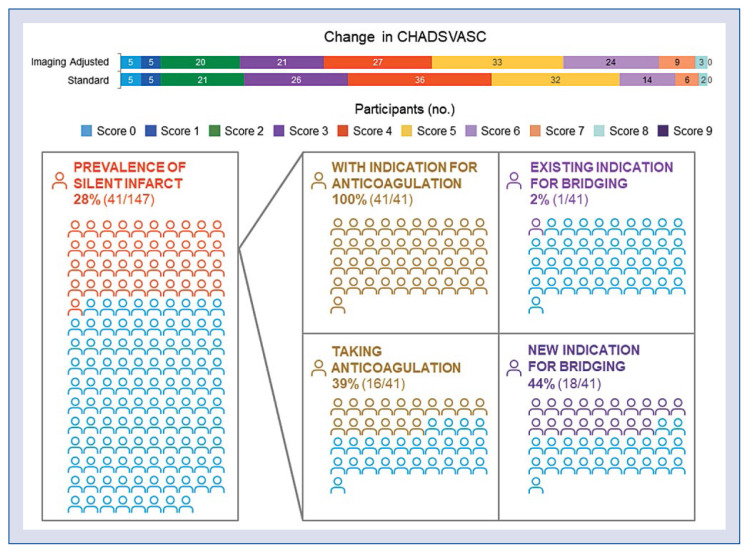
Background: The CHA2DS2-VASc score does not include silent infarcts on neuroimaging in stroke risk estimation for patients with atrial fibrillation (AF). The inclusion of silent infarcts into CHA2DS2-VASc scoring and its impact on stroke prophylaxis recommendations in patients with AF has not been previously studied. The present study sought to quantify the prevalence of silent infarcts in patients with AF and describe potential changes in management based on magnetic resonance imaging (MRI) findings.
Methods: Participants from the Mayo Clinic Study of Aging with AF and brain MRI were included. Silent infarcts were identified. "Standard" CHA2DS2-VASc scores were calculated for each subject based on clinical history alone and "imaging-adjusted" CHA2DS2-VASc scores based on evidence of cerebral infarction on MRI. Standard and imaging-adjusted scores were compared.
Results: One hundred and forty-seven participants (average age 77, 28% female) were identified with AF, MRI, and no clinical history of stroke. Overall, 41 (28%) patients had silent infarcts on MRI, corresponding with a 2-point increase in CHA2DS2-VASc score. Of these participants, only 39% (16/41) with silent infarct were on anticoagulation despite having standard CHA2DS2-VASc scores supportive of anticoagulation. After incorporating silent infarcts, 13% (19/147) would have an indication for periprocedural bridging compared to 0.6% (1/147) at baseline.
Conclusions: Incorporation of silent infarcts into the CHA2DS2-VASc score may change the risk- -benefit ratio of anticoagulation. It may also increase the number of patients who would benefit from periprocedural bridging. Future research should examine whether an anticoagulation strategy based on imaging-adjusted CHA2DS2-VASc scores could result in a greater reduction of stroke and cognitive decline.
Keywords: anticoagulation; atrial fibrillation; bridging; magnetic resonance imaging; silent infarct.
Conflict of interest statement
Figures


References
-
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation. 2019;140(2):e125–e151. doi: 10.1161/CIR.0000000000000665. - DOI - PubMed
-
- Lip GYH, Nieuwlaat R, Pisters R, et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263–272. doi: 10.1378/chest.09-1584. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
