

The effect of the COVID-19 lockdown on mental health care use in South Africa: an interrupted time-series analysis
- PMID: 35703078
- PMCID: PMC9245492
- DOI: 10.1017/S2045796022000270
The effect of the COVID-19 lockdown on mental health care use in South Africa: an interrupted time-series analysis
Abstract
Aims: The coronavirus disease 2019 (COVID-19) pandemic and ensuing restrictions have negatively affected the mental health and well-being of the general population, and there is increasing evidence suggesting that lockdowns have led to a disruption of health services. In March 2020, South Africa introduced a lockdown in response to the COVID-19 pandemic, entailing the suspension of all non-essential activities and a complete ban of tobacco and alcohol sales. We studied the effect of the lockdown on mental health care utilisation rates in private-sector care in South Africa.
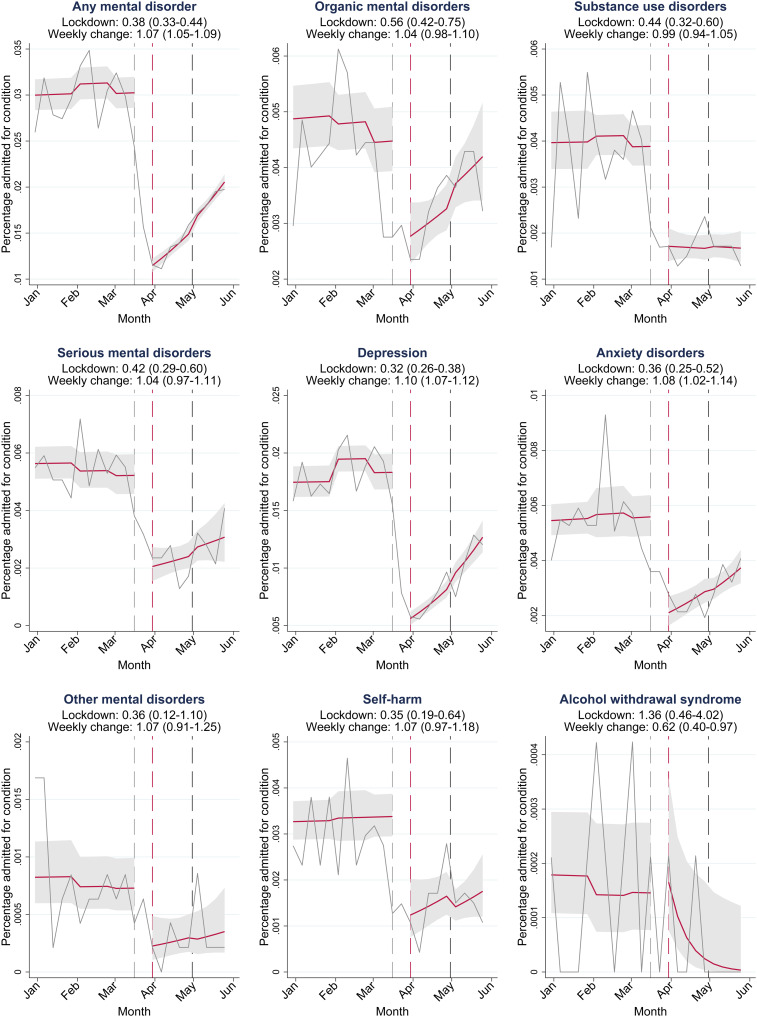
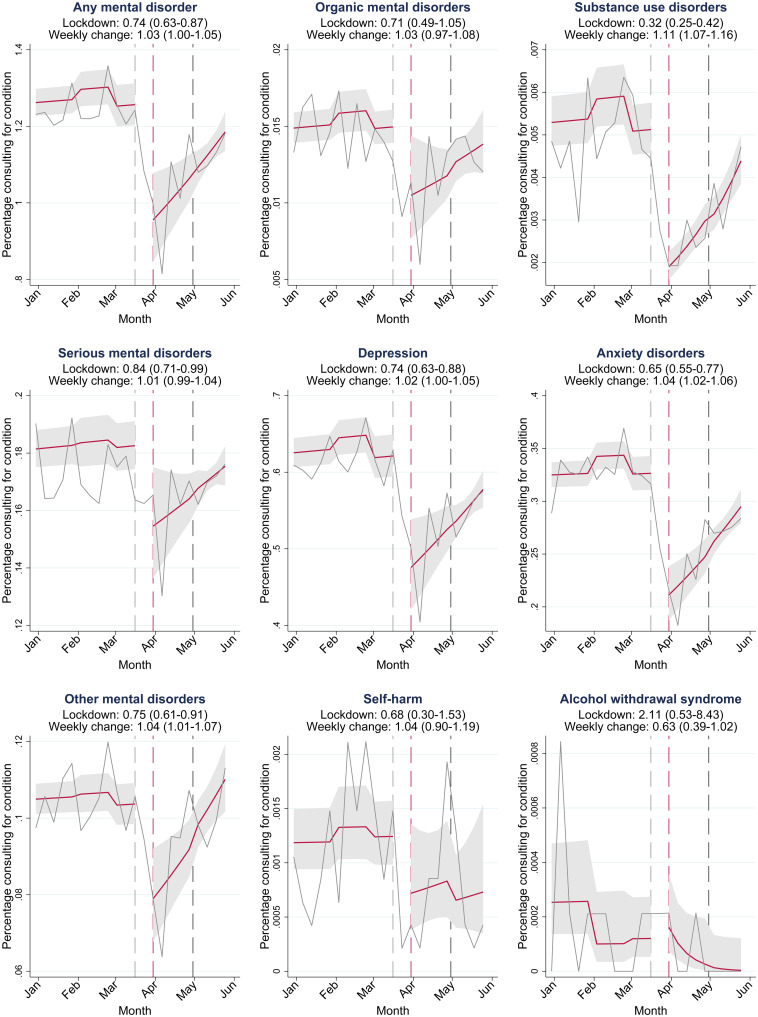
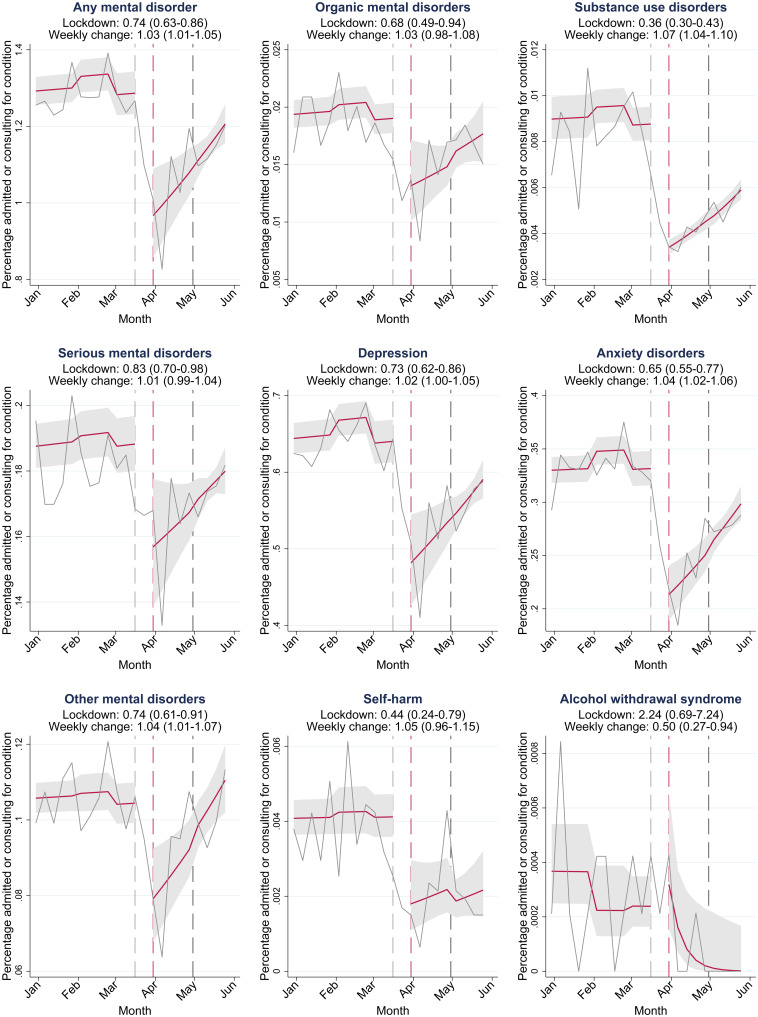
Methods: We conducted an interrupted time-series analysis using insurance claims from 1 January 2017 to 1 June 2020 of beneficiaries 18 years or older from a large private sector medical insurance scheme. We calculated weekly outpatient consultation and hospital admission rates for organic mental disorders, substance use disorders, serious mental disorders, depression, anxiety, other mental disorders, any mental disorder and alcohol withdrawal syndrome. We calculated adjusted odds ratios (OR) for the effect of the lockdown on weekly outpatient consultation and hospital admission rates and the weekly change in rates during the lockdown until 1 June 2020.
Results: 710 367 persons were followed up for a median of 153 weeks. Hospital admission rates (OR 0.38; 95% confidence interval (CI) 0.33-0.44) and outpatient consultation rates (OR 0.74; 95% CI 0.63-0.87) for any mental disorder decreased substantially after the introduction of the lockdown and did not recover to pre-lockdown levels by 1 June 2020. Health care utilisation rates for alcohol withdrawal syndrome doubled after the introduction of the lockdown, but the statistical uncertainty around the estimates was large (OR 2.24; 95% CI 0.69-7.24).
Conclusions: Mental health care utilisation rates for inpatient and outpatient services decreased substantially after the introduction of the lockdown. Hospital admissions and outpatient consultations for alcohol withdrawal syndrome increased after the introduction of the lockdown, but statistical uncertainty precludes strong conclusions about a potential unintended effect of the alcohol sales ban. Governments should integrate strategies for ensuring access and continuity of essential mental health services during lockdowns in pandemic preparedness planning.
Keywords: Alcohol abuse; health service research; psychiatric hospital; psychiatric services.
Conflict of interest statement
None.
Figures
Similar articles
-
Impact of the COVID-19 pandemic on health-care use among patients with cancer in England, UK: a comprehensive phase-by-phase time-series analysis across attendance types for 38 cancers.Lancet Digit Health. 2024 Oct;6(10):e691-e704. doi: 10.1016/S2589-7500(24)00152-3. Lancet Digit Health. 2024. PMID: 39332853
-
COVID 19-impact on substance use treatment utilization and provision in South Africa.Subst Abuse Treat Prev Policy. 2022 Mar 3;17(1):15. doi: 10.1186/s13011-022-00446-6. Subst Abuse Treat Prev Policy. 2022. PMID: 35241095 Free PMC article.
-
The Effects of COVID-19 Pandemic Lockdowns on Alcohol Consumption and Tobacco Smoking Behaviour in South Africa: A National Survey.Eur Addict Res. 2023;29(2):127-140. doi: 10.1159/000528484. Epub 2023 Mar 17. Eur Addict Res. 2023. PMID: 36934716 Free PMC article.
-
Prohibiting alcohol sales during the coronavirus disease 2019 pandemic has positive effects on health services in South Africa.Afr J Prim Health Care Fam Med. 2020 Jul 15;12(1):e1-e4. doi: 10.4102/phcfm.v12i1.2528. Afr J Prim Health Care Fam Med. 2020. PMID: 32787395 Free PMC article. Review.
-
[Utilization of mental health services in Germany during the first year of the COVID-19 pandemic-Systematic review and meta-analysis].Nervenarzt. 2025 May;96(3):257-265. doi: 10.1007/s00115-025-01812-y. Epub 2025 Mar 7. Nervenarzt. 2025. PMID: 40053131 Free PMC article. German.
Cited by
-
The Impact of COVID-19 on Mental Healthcare Utilization in Switzerland Was Strongest Among Young Females-Retrospective Study in 2018-2020.Int J Public Health. 2023 May 19;68:1605839. doi: 10.3389/ijph.2023.1605839. eCollection 2023. Int J Public Health. 2023. PMID: 37273771 Free PMC article.
-
Effect of the Friendship Bench intervention on antiretroviral therapy outcomes and mental health symptoms in rural Zimbabwe: A cluster randomized trial.medRxiv [Preprint]. 2023 Jan 22:2023.01.21.23284784. doi: 10.1101/2023.01.21.23284784. medRxiv. 2023. Update in: JAMA Netw Open. 2023 Jul 3;6(7):e2323205. doi: 10.1001/jamanetworkopen.2023.23205. PMID: 36711671 Free PMC article. Updated. Preprint.
-
Residential and inpatient treatment of substance use disorders in Sub-Saharan Africa: a scoping review.Subst Abuse Treat Prev Policy. 2024 Jan 11;19(1):6. doi: 10.1186/s13011-023-00589-0. Subst Abuse Treat Prev Policy. 2024. PMID: 38212834 Free PMC article.
-
Effect of COVID-19 pandemic on serious mental illness-related outpatient department utilization in Ningbo, China: an interrupted time series analysis.Front Psychiatry. 2023 Jul 13;14:1199408. doi: 10.3389/fpsyt.2023.1199408. eCollection 2023. Front Psychiatry. 2023. PMID: 37520234 Free PMC article.
-
Impact of COVID-19 pandemic on depression incidence and healthcare service use among patients with depression: an interrupted time-series analysis from a 9-year population-based study.BMC Med. 2024 Apr 22;22(1):169. doi: 10.1186/s12916-024-03386-z. BMC Med. 2024. PMID: 38644506 Free PMC article.
References
-
- Altamura AC, Dell'Osso B, Berlin HA, Buoli M, Bassetti R and Mundo E (2010) Duration of untreated illness and suicide in bipolar disorder: a naturalistic study. European Archives of Psychiatry and Clinical Neuroscience 260, 385–391. - PubMed
-
- Benatti B, Camuri G, Dell'Osso B, Cremaschi L, Sembira E, Palazzo C, Oldani L, Dobrea C, Arici C, Primavera D, Carpiniello B, Castellano F, Carrà G, Clerici M, Baldwin DS and Altamura AC (2016) Which factors influence onset and latency to treatment in generalized anxiety disorder, panic disorder, and obsessive-compulsive disorder? International Clinical Psychopharmacology 31, 347–352. - PubMed
-
- Boldrini T, Girardi P, Clerici M, Conca A, Creati C, Di Cicilia G, Ducci G, Durbano F, Maci C, Maone A, Nicolò G, Oasi O, Percudani M, Polselli GM, Pompili M, Rossi A, Salcuni S, Tarallo F, Vita A and Lingiardi V (2021) Consequences of the COVID-19 pandemic on admissions to general hospital psychiatric wards in Italy: reduced psychiatric hospitalizations and increased suicidality. Progress in Neuro-Psychopharmacology and Biological Psychiatry 110, 110304. - PMC - PubMed
-
- Council for Medical Schemes (2020) Annual Report Council for Medical Schemes. Hatfield: Council for Medical Schemes.
