

Association of Sitting Time With Mortality and Cardiovascular Events in High-Income, Middle-Income, and Low-Income Countries
- PMID: 35704349
- PMCID: PMC9201743
- DOI: 10.1001/jamacardio.2022.1581
Association of Sitting Time With Mortality and Cardiovascular Events in High-Income, Middle-Income, and Low-Income Countries
Abstract
Importance: High amounts of sitting time are associated with increased risks of cardiovascular disease (CVD) and mortality in high-income countries, but it is unknown whether risks also increase in low- and middle-income countries.
Objective: To investigate the association of sitting time with mortality and major CVD in countries at different economic levels using data from the Prospective Urban Rural Epidemiology study.
Design, setting, and participants: This population-based cohort study included participants aged 35 to 70 years recruited from January 1, 2003, and followed up until August 31, 2021, in 21 high-income, middle-income, and low-income countries with a median follow-up of 11.1 years.
Exposures: Daily sitting time measured using the International Physical Activity Questionnaire.
Main outcomes and measures: The composite of all-cause mortality and major CVD (defined as cardiovascular death, myocardial infarction, stroke, or heart failure).
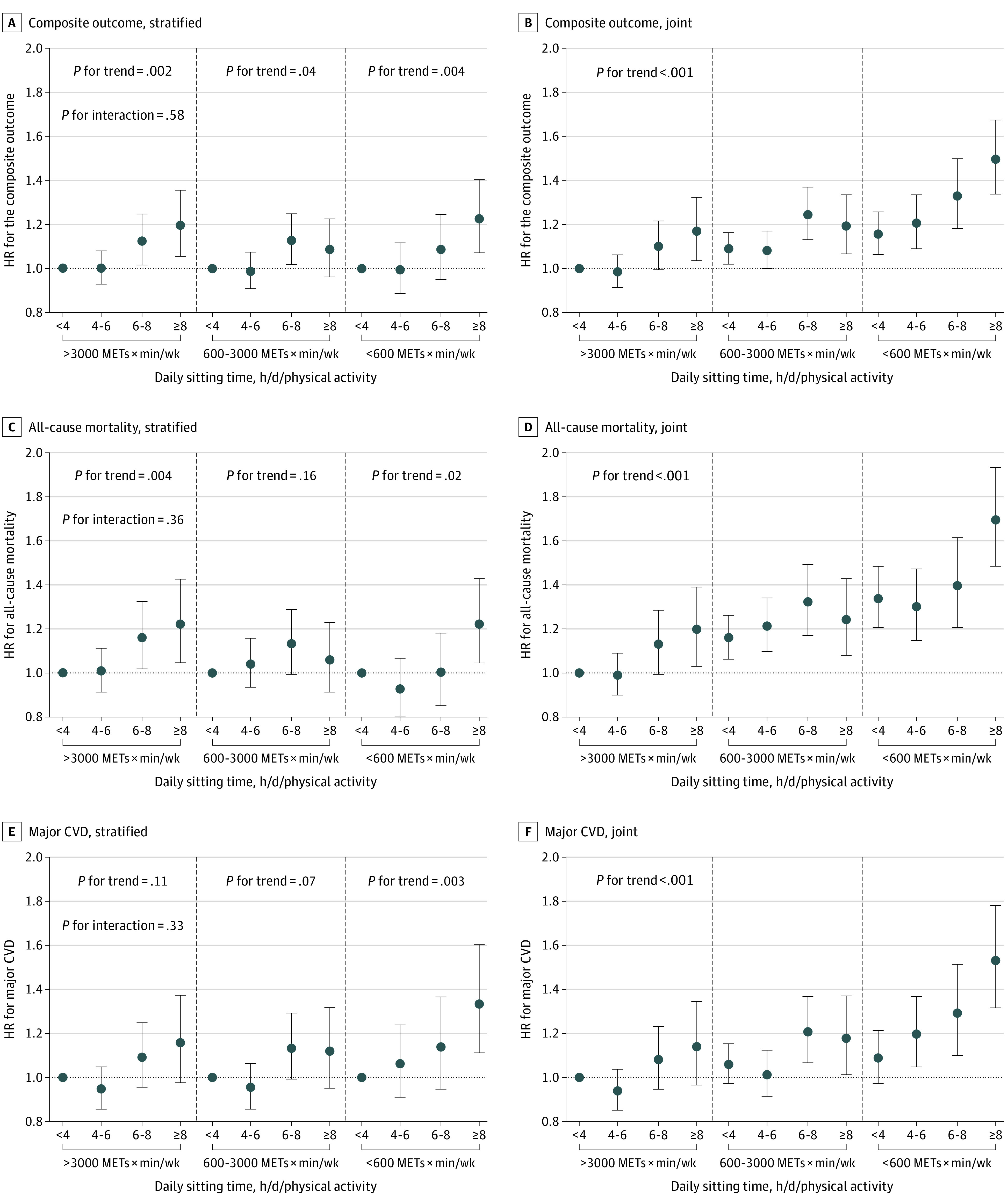
Results: Of 105 677 participants, 61 925 (58.6%) were women, and the mean (SD) age was 50.4 (9.6) years. During a median follow-up of 11.1 (IQR, 8.6-12.2) years, 6233 deaths and 5696 major cardiovascular events (2349 myocardial infarctions, 2966 strokes, 671 heart failure, and 1792 cardiovascular deaths) were documented. Compared with the reference group (<4 hours per day of sitting), higher sitting time (≥8 hours per day) was associated with an increased risk of the composite outcome (hazard ratio [HR], 1.19; 95% CI, 1.11-1.28; Pfor trend < .001), all-cause mortality (HR, 1.20; 95% CI, 1.10-1.31; Pfor trend < .001), and major CVD (HR, 1.21; 95% CI, 1.10-1.34; Pfor trend < .001). When stratified by country income levels, the association of sitting time with the composite outcome was stronger in low-income and lower-middle-income countries (≥8 hours per day: HR, 1.29; 95% CI, 1.16-1.44) compared with high-income and upper-middle-income countries (HR, 1.08; 95% CI, 0.98-1.19; P for interaction = .02). Compared with those who reported sitting time less than 4 hours per day and high physical activity level, participants who sat for 8 or more hours per day experienced a 17% to 50% higher associated risk of the composite outcome across physical activity levels; and the risk was attenuated along with increased physical activity levels.
Conclusions and relevance: High amounts of sitting time were associated with increased risk of all-cause mortality and CVD in economically diverse settings, especially in low-income and lower-middle-income countries. Reducing sedentary time along with increasing physical activity might be an important strategy for easing the global burden of premature deaths and CVD.
Conflict of interest statement
Figures


References
-
- Du Y, Liu B, Sun Y, Snetselaar LG, Wallace RB, Bao W. Trends in adherence to the physical activity guidelines for Americans for aerobic activity and time spent on sedentary behavior among US adults, 2007-2016. JAMA Netw Open. 2019;2(7):e197597. doi:10.1001/jamanetworkopen.2019.7597 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
