

Treatment of Anal High-Grade Squamous Intraepithelial Lesions to Prevent Anal Cancer
- PMID: 35704479
- PMCID: PMC9717677
- DOI: 10.1056/NEJMoa2201048
Treatment of Anal High-Grade Squamous Intraepithelial Lesions to Prevent Anal Cancer
Abstract
Background: The incidence of anal cancer is substantially higher among persons living with the human immunodeficiency virus (HIV) than in the general population. Similar to cervical cancer, anal cancer is preceded by high-grade squamous intraepithelial lesions (HSILs). Treatment for cervical HSIL reduces progression to cervical cancer; however, data from prospective studies of treatment for anal HSIL to prevent anal cancer are lacking.
Methods: We conducted a phase 3 trial at 25 U.S. sites. Persons living with HIV who were 35 years of age or older and who had biopsy-proven anal HSIL were randomly assigned, in a 1:1 ratio, to receive either HSIL treatment or active monitoring without treatment. Treatment included office-based ablative procedures, ablation or excision under anesthesia, or the administration of topical fluorouracil or imiquimod. The primary outcome was progression to anal cancer in a time-to-event analysis. Participants in the treatment group were treated until HSIL was completely resolved. All the participants underwent high-resolution anoscopy at least every 6 months; biopsy was also performed for suspected ongoing HSIL in the treatment group, annually in the active-monitoring group, or any time there was concern for cancer.
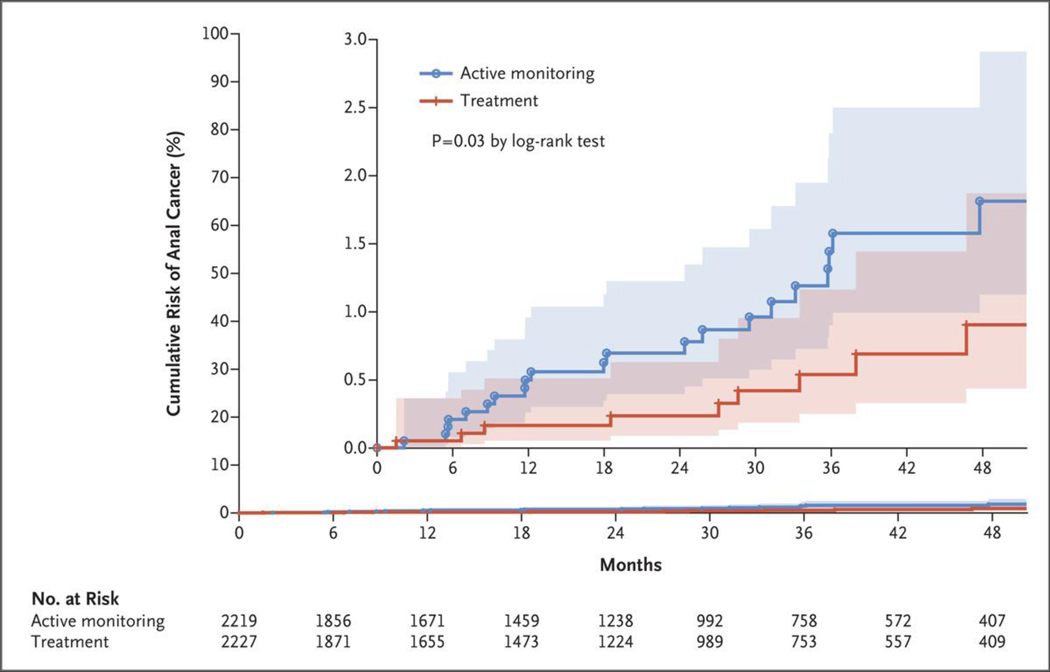
Results: Of 4459 participants who underwent randomization, 4446 (99.7%) were included in the analysis of the time to progression to cancer. With a median follow-up of 25.8 months, 9 cases were diagnosed in the treatment group (173 per 100,000 person-years; 95% confidence interval [CI], 90 to 332) and 21 cases in the active-monitoring group (402 per 100,000 person-years; 95% CI, 262 to 616). The rate of progression to anal cancer was lower in the treatment group than in the active-monitoring group by 57% (95% CI, 6 to 80; P = 0.03 by log-rank test).
Conclusions: Among participants with biopsy-proven anal HSIL, the risk of anal cancer was significantly lower with treatment for anal HSIL than with active monitoring. (Funded by the National Cancer Institute; ClinicalTrials.gov number, NCT02135419.).
Copyright © 2022 Massachusetts Medical Society.
Figures

Comment in
-
Prevention of Anal Cancer.N Engl J Med. 2022 Aug 18;387(7):665. doi: 10.1056/NEJMc2209237. N Engl J Med. 2022. PMID: 36070724 No abstract available.
-
Prevention of Anal Cancer.N Engl J Med. 2022 Aug 18;387(7):665-666. doi: 10.1056/NEJMc2209237. N Engl J Med. 2022. PMID: 36070725 No abstract available.
-
Prevention of Anal Cancer.N Engl J Med. 2022 Aug 18;387(7):666. doi: 10.1056/NEJMc2209237. N Engl J Med. 2022. PMID: 36070726 No abstract available.
References
-
- Hoots BE, Palefsky JM, Pimenta JM, Smith JS. Human papillomavirus type distribution in anal cancer and anal intraepithelial lesions. Int J Cancer 2009; 124:2375–83. - PubMed
-
- Berry JM, Jay N, Cranston RD, et al. Progression of anal high-grade squamous intraepithelial lesions to invasive anal cancer among HIV-infected men who have sex with men. Int J Cancer 2014;134:1147–55. - PubMed
-
- Sand FL, Munk C, Jensen SM, Svahn MF, Frederiksen K, Kjær SK. Long-term risk for noncervical anogenital cancer in women with previously diagnosed high-grade cervical intraepithelial neoplasia: a Danish nationwide cohort study. Cancer Epidemiol Biomarkers Prev 2016;25:1090–7. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical