

Sequential Stem Cell-Kidney Transplantation in Schimke Immuno-osseous Dysplasia
- PMID: 35704481
- PMCID: PMC10545450
- DOI: 10.1056/NEJMoa2117028
Sequential Stem Cell-Kidney Transplantation in Schimke Immuno-osseous Dysplasia
Abstract
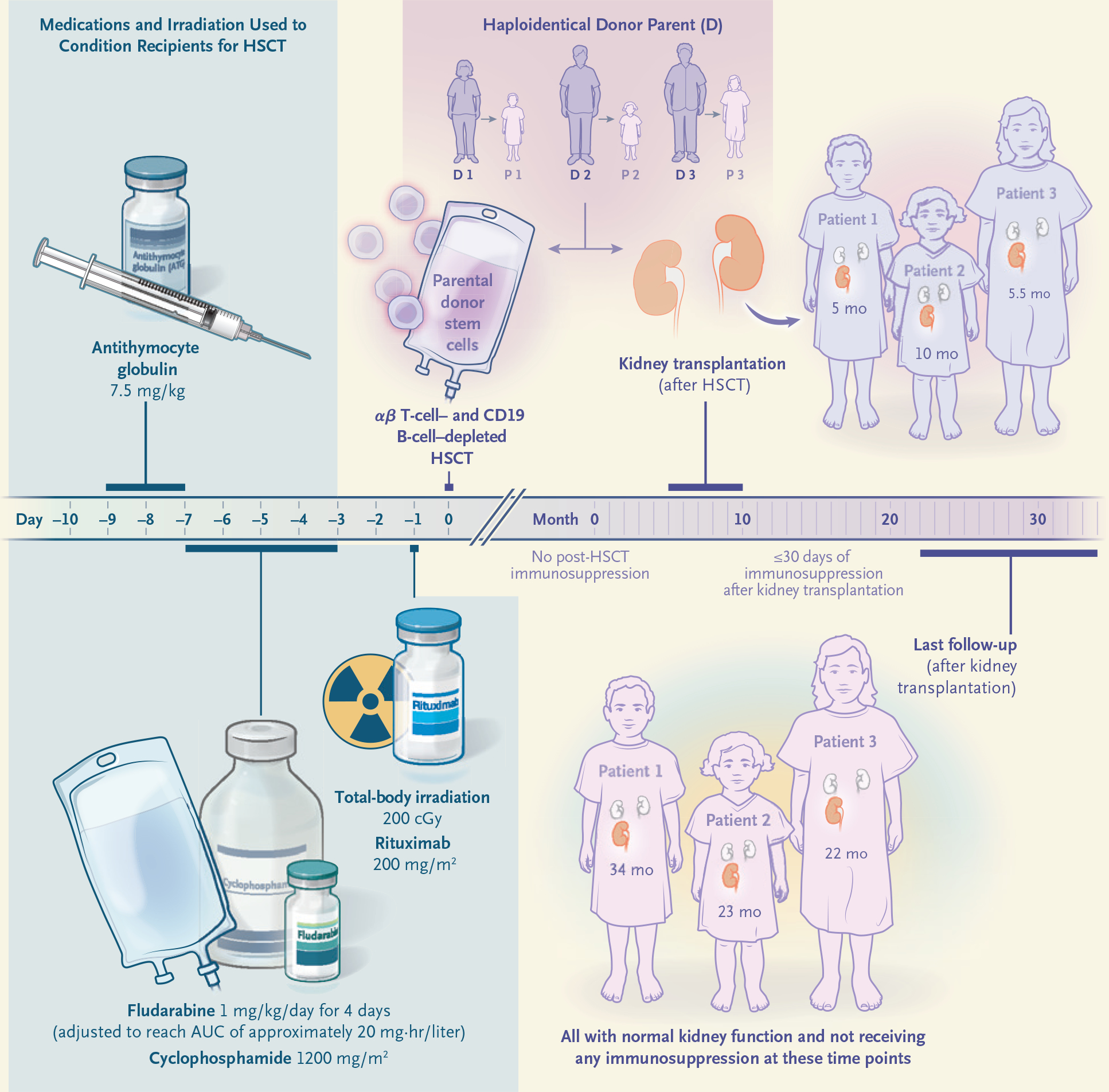
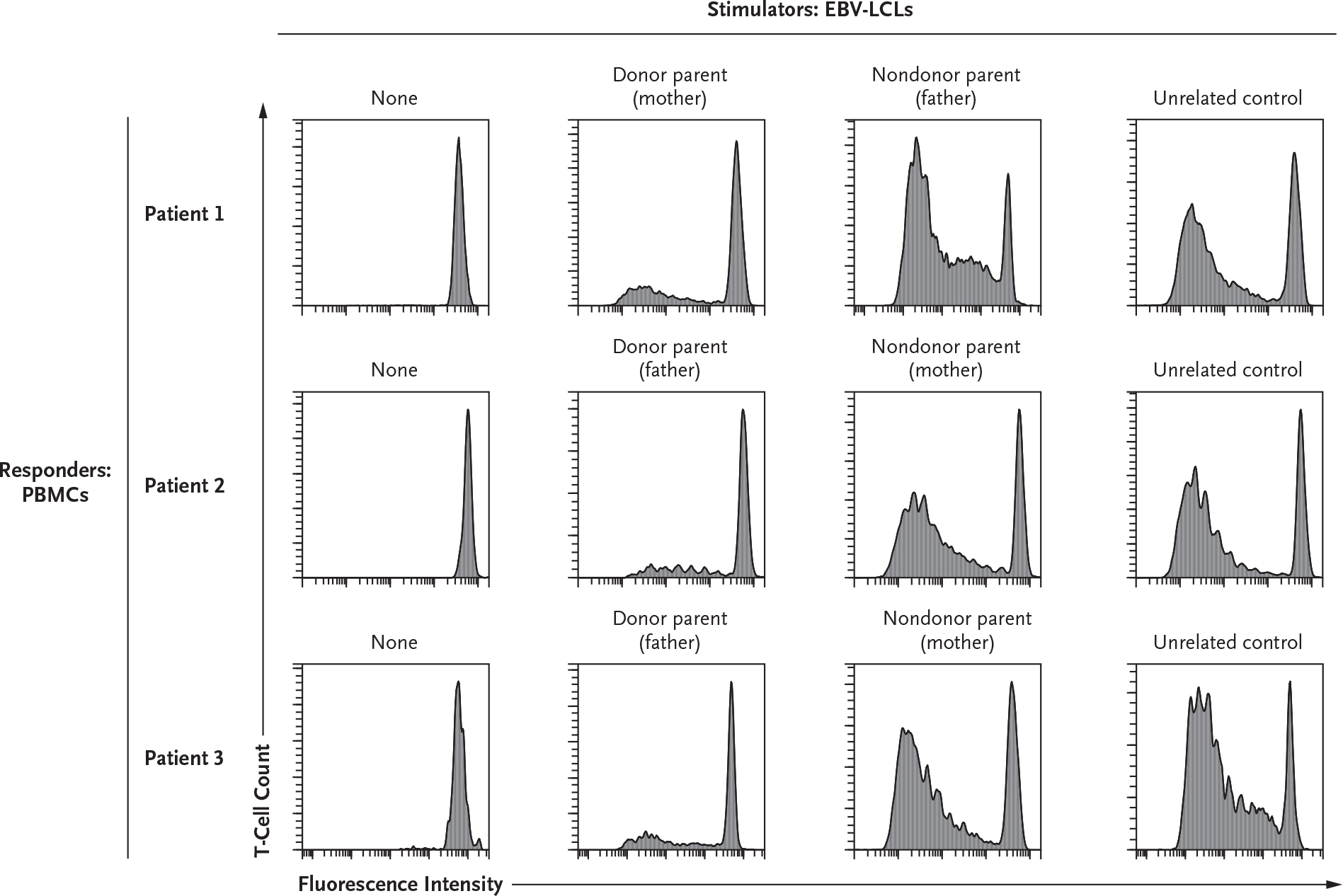
Lifelong immunosuppression is required for allograft survival after kidney transplantation but may not ultimately prevent allograft loss resulting from chronic rejection. We developed an approach that attempts to abrogate immune rejection and the need for post-transplantation immunosuppression in three patients with Schimke immuno-osseous dysplasia who had both T-cell immunodeficiency and renal failure. Each patient received sequential transplants of αβ T-cell-depleted and CD19 B-cell-depleted haploidentical hematopoietic stem cells and a kidney from the same donor. Full donor hematopoietic chimerism and functional ex vivo T-cell tolerance was achieved, and the patients continued to have normal renal function without immunosuppression at 22 to 34 months after kidney transplantation. (Funded by the Kruzn for a Kure Foundation.).
Copyright © 2022 Massachusetts Medical Society.
Figures
Comment in
-
Transplantation Tolerance through Hematopoietic Chimerism.N Engl J Med. 2022 Jun 16;386(24):2332-2333. doi: 10.1056/NEJMe2204651. N Engl J Med. 2022. PMID: 35704487 No abstract available.
-
Sequential Stem Cell-Kidney Transplantation in Schimke Immuno-osseous Dysplasia.N Engl J Med. 2022 Sep 1;387(9):859. doi: 10.1056/NEJMc2209527. N Engl J Med. 2022. PMID: 36053525 No abstract available.
References
-
- Poggio ED, Augustine JJ, Arrigain S, Brennan DC, Schold JD. Long-term kidney transplant graft survival — making progress when most needed. Am J Transplant 2021;21:2824–32. - PubMed
-
- Leventhal JR, Ildstad ST. Tolerance induction in HLA disparate living donor kidney transplantation by facilitating cell-enriched donor stem cell Infusion: the importance of durable chimerism. Hum Immunol 2018;79:272–6. - PubMed
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical