

Referral challenges and outcomes of neonates received at Muhimbili National Hospital, Dar es Salaam, Tanzania
- PMID: 35704624
- PMCID: PMC9200315
- DOI: 10.1371/journal.pone.0269479
Referral challenges and outcomes of neonates received at Muhimbili National Hospital, Dar es Salaam, Tanzania
Abstract
Background: Functional referral system including pre referral care, access to emergency transport and ensuring continuity of care between facilities is critical for improved newborn health outcome. The neonatal transport system is quite undervalued in many sub Saharan countries, Tanzania included. This study assessed the pre referral care, transport process, ambulance characteristics, admission clinical status and outcomes of referred neonates at Muhimbili National Hospital Upanga, a tertiary facility in Dar es Salaam, Tanzania.
Methods: A descriptive cross sectional study with a longitudinal follow up was conducted from September 2020 to February 2021 including neonates referred to Muhimbili National Hospital. A structured questionnaire was used to collect demographic characteristics and transport factors including pre referral care extracted from the referral documents and through interviewing caregivers or escorting person/nurse. Ambulances were directly observed using a structured checklist on presence, absence and functionality of supportive equipment. All enrolled neonates had a clinical assessment at admission and 48 hours post admission to determine admission clinical status and 48 hours' clinical outcome as either survived/died.
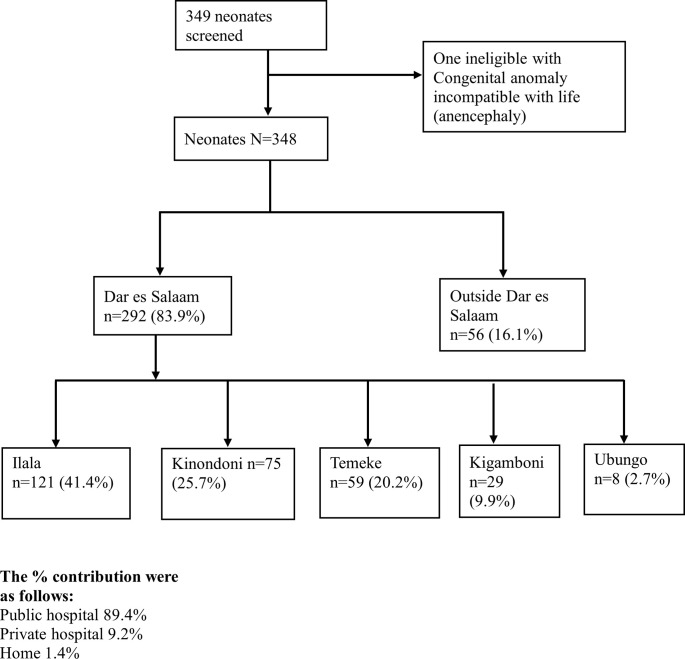
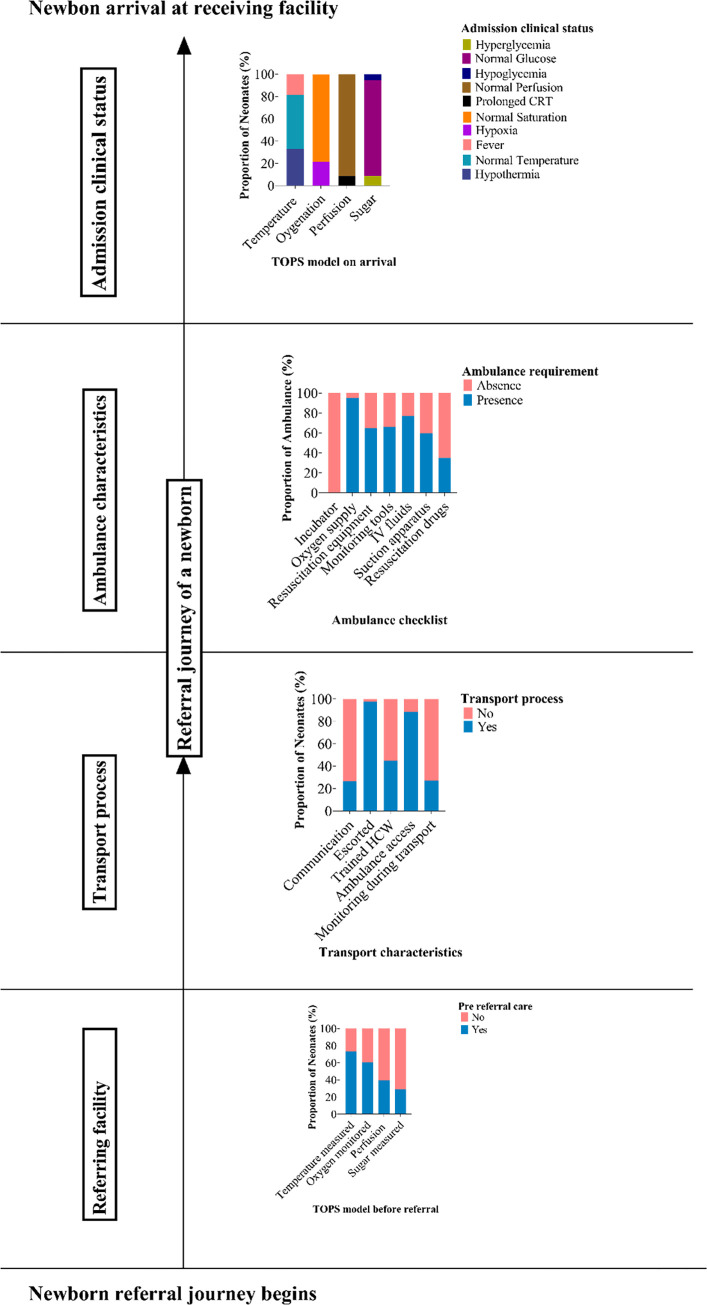
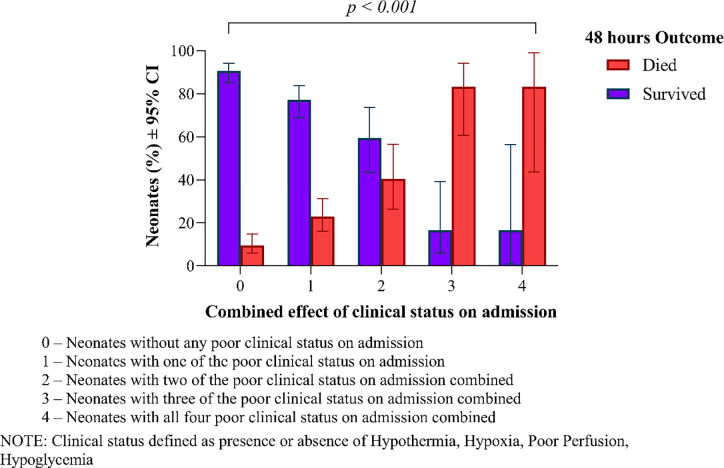
Results: Out of the 348 neonates assessed during the study period, the median gestation age was 38 weeks (IQR 32, 39) with the mean birth weight of 2455 ± 938 g. Pre referral documentation showed that temperature was measured in 176 (57.1%), oxygen saturation and random blood glucose in only 143 (46.6%) and 116 (36.2%) neonates respectively. Ambulance was used as a means of transportation in 308 (88.5%) neonates. While no ambulance had an incubator only 7 (2.0%) neonates were kept on a Kangaroo Mother Care position. Monitoring enroute was done to only 94 (27%) of the transferred neonates with 169 (54.9%) of health care professionals escorting the neonates lacking training on essential newborn care. On arrival, 115 (33%) were hypothermic, 74 (21.3%) hypoxic, 30 (8.6%) with poor perfusion and 49 (14.1%) hypoglycemic. Hypothermic neonates had an increased chance of dying compared to those who were normothermic (OR = 2.09, 95% CI (1.05-4.20), p = 0.037). The chance of dying among those presenting with hypoxia was almost three times (OR = 2.88, 95%CI (1.44-5.74), p = 0.003) while those with poor perfusion was almost five times (OR = 4.76, 95%CI (1.80-12.58), p = 0.002). Additionally, neonates who had hyperglycemia (RBG > 8.3mmol/l) on arrival had a higher probability of dying compared to those who were euglycemic [(OR = 3.10, 95% CI (1.19-8.09) p = 0.021]. Overall mortality was 22.4% within 48 hours of admission and risk of dying increased as the presence of poor clinical status added on.
Conclusion: Neonatal transportation in Dar es Salaam, Tanzania was observed to be challenging. Pre transfer care and monitoring during transportation was inadequate and this contributed to poor clinical status on admission. Hypothermia, hypoglycemia, hyperglycemia, hypoxia and poor perfusion on admission were associated with increased mortality. Effective referral network is needed for improved neonatal health outcomes. Pre referral supportive care, training of health care professionals, transportation with improved monitoring, clear communication protocol and referral documentation should be invested and effectively utilized.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Transportation services for neonates referred to a secondary level health care facility in rural Tanzania: a cross-sectional study.J Matern Fetal Neonatal Med. 2025 Dec;38(1):2458595. doi: 10.1080/14767058.2025.2458595. Epub 2025 Feb 2. J Matern Fetal Neonatal Med. 2025. PMID: 39894465
-
Neonatal hypothermia on admission to a special care unit in Dar-es-Salaam, Tanzania: a cause for concern.Cent Afr J Med. 2003 Mar-Apr;49(3-4):23-7. Cent Afr J Med. 2003. PMID: 14562586
-
Poor weight gain and its predictors among preterm neonates admitted at Muhimbili National Hospital in Dar-es-salaam, Tanzania: a prospective cohort study.BMC Pediatr. 2021 Nov 6;21(1):493. doi: 10.1186/s12887-021-02971-y. BMC Pediatr. 2021. PMID: 34740360 Free PMC article.
-
Incidence and determinants of perinatal mortality in five urban hospitals in Dar es Salaam, Tanzania: a cohort study with an embedded case-control analysis.BMC Pregnancy Childbirth. 2024 Jan 13;24(1):62. doi: 10.1186/s12884-023-06096-1. BMC Pregnancy Childbirth. 2024. PMID: 38218766 Free PMC article.
-
Predictors and outcome of time to presentation among critically ill paediatric patients at Emergency Department of Muhimbili National Hospital, Dar es Salaam, Tanzania.BMC Pediatr. 2022 Jul 22;22(1):441. doi: 10.1186/s12887-022-03503-y. BMC Pediatr. 2022. PMID: 35864482 Free PMC article.
Cited by
-
The Challenges of Implementing a Health Referral System in South Africa: A Qualitative Study.Risk Manag Healthc Policy. 2024 Apr 10;17:855-864. doi: 10.2147/RMHP.S450998. eCollection 2024. Risk Manag Healthc Policy. 2024. PMID: 38623578 Free PMC article.
-
Advancing primary care: Establishing family medicine specialty in Tanzania.Afr J Prim Health Care Fam Med. 2023 Dec 4;15(1):e1-e4. doi: 10.4102/phcfm.v%vi%i.4248. Afr J Prim Health Care Fam Med. 2023. PMID: 38044889 Free PMC article.
-
Assessment of neonatal referral infrastructure and clinical characteristics of referred neonates in three first referral hospitals in Nairobi County, Kenya.Wellcome Open Res. 2023 Nov 24;8:126. doi: 10.12688/wellcomeopenres.18871.3. eCollection 2023. Wellcome Open Res. 2023. PMID: 39507276 Free PMC article.
-
Asymptomatic hypoglycemia among preterm newborns: A cross-sectional analysis.PLoS One. 2024 Apr 30;19(4):e0301803. doi: 10.1371/journal.pone.0301803. eCollection 2024. PLoS One. 2024. PMID: 38687725 Free PMC article.
-
Predictors of neonatal hypothermia within six hours of birth and exploring preventive practices among post-natal mothers in Kilimanjaro region: Explanatory sequential mixed method protocol.PLoS One. 2024 Nov 8;19(11):e0313432. doi: 10.1371/journal.pone.0313432. eCollection 2024. PLoS One. 2024. PMID: 39514561 Free PMC article.
References
-
- MoHCDGEC. Tanzania Demorgraphic and Health Survey Indicator Survey (TDHS-MIS) 2015–2016. Dar es Salaam, Tanzania, Rockville, Maryland, USA MoHCDGEC, MoH, NBS, OCGS, ICF. 2016;1(1):1–630.
-
- World Health Organization. The Network to Improve Quality of Care for Maternal, Newborn and Child Health.; 2018.
-
- Harahap NC, Handayani PW, Hidayanto AN. Barriers and technologies of maternal and neonatal referral system in developing countries: A narrative review. Informatics Med Unlocked. 2019;15(April):100184.
-
- Mir NA, Javied S. Transport of sick neonates: practical considerations. Indian Pediatr. 1989;26:755–764. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
