

Vaccination against SARS-CoV-2 protects from morbidity, mortality and sequelae from COVID19 in patients with cancer
- PMID: 35704976
- PMCID: PMC9124924
- DOI: 10.1016/j.ejca.2022.04.036
Vaccination against SARS-CoV-2 protects from morbidity, mortality and sequelae from COVID19 in patients with cancer
Abstract
Background: Although SARS-CoV-2 vaccines immunogenicity in patients with cancer has been investigated, whether they can significantly improve the severity of COVID-19 in this specific population is undefined.
Methods: Capitalizing on OnCovid (NCT04393974) registry data we reported COVID-19 mortality and proxies of COVID-19 morbidity, including post-COVID-19 outcomes, according to the vaccination status of the included patients.
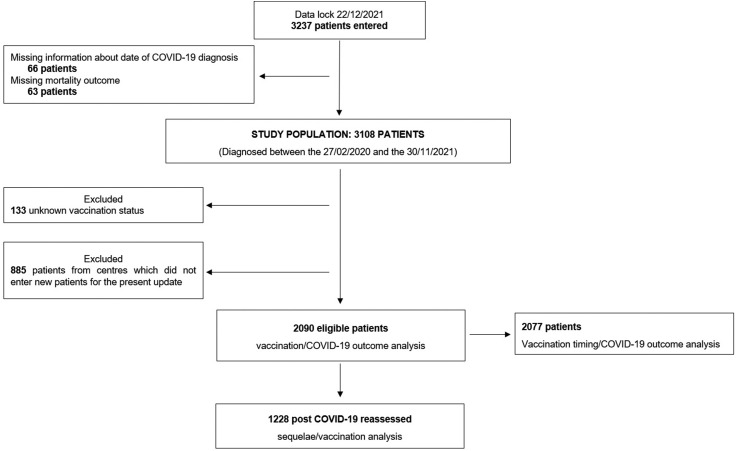
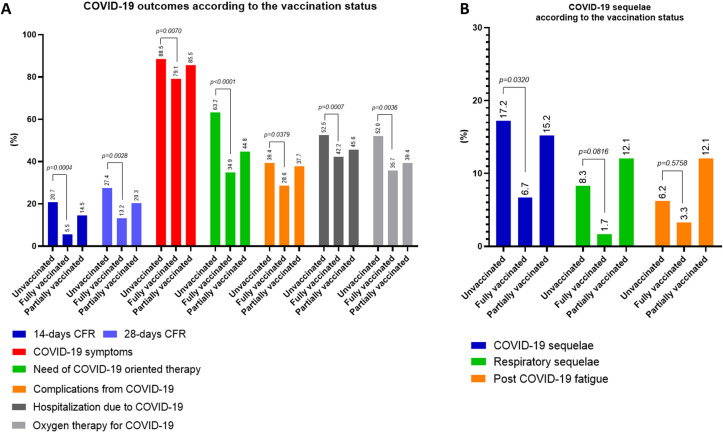
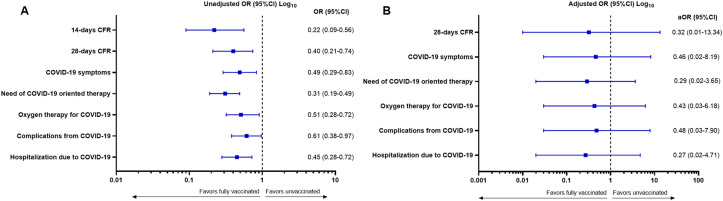
Results: 2090 eligible patients diagnosed with COVID-19 between 02/2020 and 11/2021 were included, of whom 1930 (92.3%) unvaccinated, 91 (4.4%) fully vaccinated and 69 (3.3%) partially vaccinated. With the exception of a higher prevalence of patients from the UK (p = 0.0003) and receiving systemic anticancer therapy at COVID-19 diagnosis (p = 0.0082) among fully vaccinated patients, no demographics/oncological features were associated with vaccination status. The 14-days case fatality rate (CFR) (5.5% vs 20.7%, p = 0.0004) and the 28-days CFR (13.2% vs 27.4%, p = 0.0028) demonstrated a significant improvement for fully vaccinated patients in comparison with unvaccinated patients. The receipt of prior full vaccination was also associated with reduced symptomatic COVID-19 (79.1% vs 88.5%, p = 0.0070), need of COVID-19 oriented therapy (34.9% vs 63.2%, p < 0.0001), complications from COVID-19 (28.6% vs 39.4%, p = 0.0379), hospitalizations due to COVID-19 (42.2% vs 52.5%, p = 0.0007) and oxygen therapy requirement (35.7% vs 52%, p = 0.0036). Following Inverse Probability Treatment Weighting (IPTW) procedure no statistically significant difference according to the vaccination status was confirmed; however, all COVID-19 related outcomes were concordantly in favour of full vaccination. Among the 1228 (58.8%) patients who underwent a formal reassessment at participating centres after COVID-19 resolution, fully vaccinated patients experienced less sequelae than unvaccinated patients (6.7% vs 17.2%, p = 0.0320).
Conclusions: This analysis provides initial evidence in support of the beneficial effect of SARS-CoV-2 vaccines against morbidity and mortality from COVID-19 in patients with cancer.
Keywords: COVID-19; Cancer; Clinical efficacy; Prevention; SARS-CoV-2; Vaccines.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest statement The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: As corresponding author of the abovementioned manuscript, I declare on behalf of my co-authors the following conflict of interests: David J Pinato received lecture fees from ViiV Healthcare, Bayer Healthcare, BMS, Roche, EISAI, Falk Foundation, travel expenses from BMS and Bayer Healthcare; consulting fees for Mina Therapeutics, EISAI, Roche, DaVolterra and Astra Zeneca; research funding (to institution) from MSD and BMS.Aleix Prat has declared personal honoraria from Pfizer, Roche, MSD Oncology, Eli Lilly, and Daiichi Sankyo; travel, accommodations, and expenses paid by Daiichi Sankyo; research funding from Roche and Novartis; and consulting/advisory role for NanoString Technologies, Amgen, Roche, Novartis, Pfizer and Bristol-Myers Squibb.Matteo Lambertini acted as consultant for Roche, Novartis, Lilly, AstraZeneca, Exact Sciences, MSD, Pfizer, Seagen and received speaker honoraria from Roche, Novartis, Lilly, Pfizer, Takeda, Ipsen and Sandoz outside the submitted work.Joan Brunet has declared consulting/advisory role for MSD and Astra Zeneca.Alessandra Gennari has declared consulting/advisory role for Roche, MSD, Eli Lilly, Pierre Fabre, EISAI, and Daichii Sankyo; speakers bureau for Eisai, Novartis, Eli Lilly, Roche, Teva, Gentili, Pfizer, Astra Zeneca, Celgene, and Daichii Sankyo; research funds: EISAI, Eli Lilly, and Roche. CMV has received travel grants and other honoraria from BMS, MSD, Novartis and Roche.Gianluca Gaidano has declared consulting/advisory role for Janssen, Abbvie, Astra-Zeneca and BeiGene, and speaker fees from Janssen and Abbvie.Lorenza Rimassa received consulting fees from Taiho Oncology, Servier, Amgen, ArQule, AstraZeneca, Basilea, Bayer, BMS, Celgene, Eisai, Exelixis, Genenta, Hengrui, Incyte, Ipsen, IQVIA, Lilly, MSD, Nerviano Medical Sciences, Roche, Sanofi, Zymeworks; lecture fees from AbbVie, Amgen, Bayer, Eisai, Gilead, Incyte, Ipsen, Lilly, Merck Serono, Roche, Sanofi; travel expenses from Ipsen; and institutional research funding from Agios, ARMO BioSciences, AstraZeneca, BeiGene, Eisai, Exelixis, Fibrogen, Incyte, Ipsen, Lilly, MSD, Nerviano Medical Sciences, Roche, Zymeworks.Joseph Tabernero reported consulting fees from Array Biopharma, AstraZeneca, Avvinity, Bayer, Boehringer Ingelheim, Chugai, Daiichi Sankyo, F. Hoffmann-La Roche Ltd, Genentech Inc, HalioDX SAS, Hutchison MediPharma International, Ikena Oncology, Inspirna Inc, IQVIA, Lilly, Menarini, Merck Serono, Merus, MSD, Mirati, Neophore, Novartis, Ona Therapeutics, Orion Biotechnology, Peptomyc, Pfizer, Pierre Fabre, Samsung Bioepis, Sanofi, Seattle Genetics, Scandion Oncology, Servier, Sotio Biotech, Taiho, Tessa Therapeutics and TheraMyc. He also reported speaker's fees from Imedex, Medscape Education, MJH Life Sciences, PeerView Institute for Medical Education and Physicians Education Resource (PER). He also declared institutional research support from Amgen Inc, Array Biopharma Inc, AstraZeneca Pharmaceuticals LP, BeiGene, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Debiopharm International SA, F. Hoffmann-La Roche Ltd, Genentech Inc, HalioDX SAS, Hutchison MediPharma International, Janssen-Cilag SA, MedImmune, Menarini, Merck Health KGAA, Merck Sharp & Dohme, Merus NV, Mirati, Novartis Farmacéutica SA, Pfizer, Pharma Mar, Sanofi Aventis Recherche & Développement, Servier, Taiho Pharma USA Inc, Spanish Association Against Cancer Scientific Foundation and Cancer Research UK.Alessio Cortellini received consulting fees from MSD, BMS, AstraZeneca, Roche; speakers' fee from AstraZeneca, MSD, Novartis and Eisai.All remaining authors have declared no conflicts of interest.London, April 18th, 2022.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
