

Intra-abdominal septic complications after ileocolic resection increases risk for endoscopic and surgical postoperative Crohn's disease recurrence
- PMID: 35705188
- PMCID: PMC9924045
- DOI: 10.1093/ecco-jcc/jjac078
Intra-abdominal septic complications after ileocolic resection increases risk for endoscopic and surgical postoperative Crohn's disease recurrence
Abstract
Background: Postoperative recurrence [POR] of Crohn's disease following ileocolonic resection is common. The impact of immediate postoperative intra-abdominal septic complications [IASC] on endoscopic and surgical recurrence has not been elucidated.
Aims: To evaluate if IASC is associated with an increased risk for endoscopic and surgical POR.
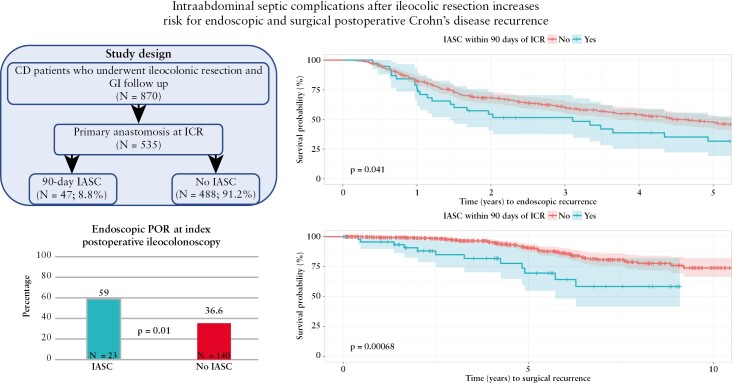
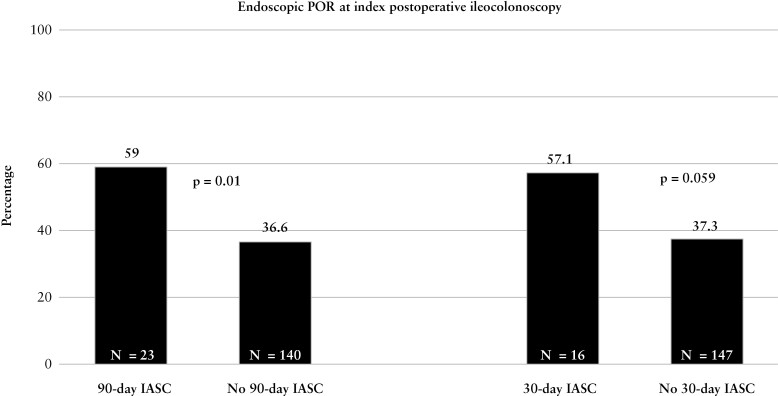
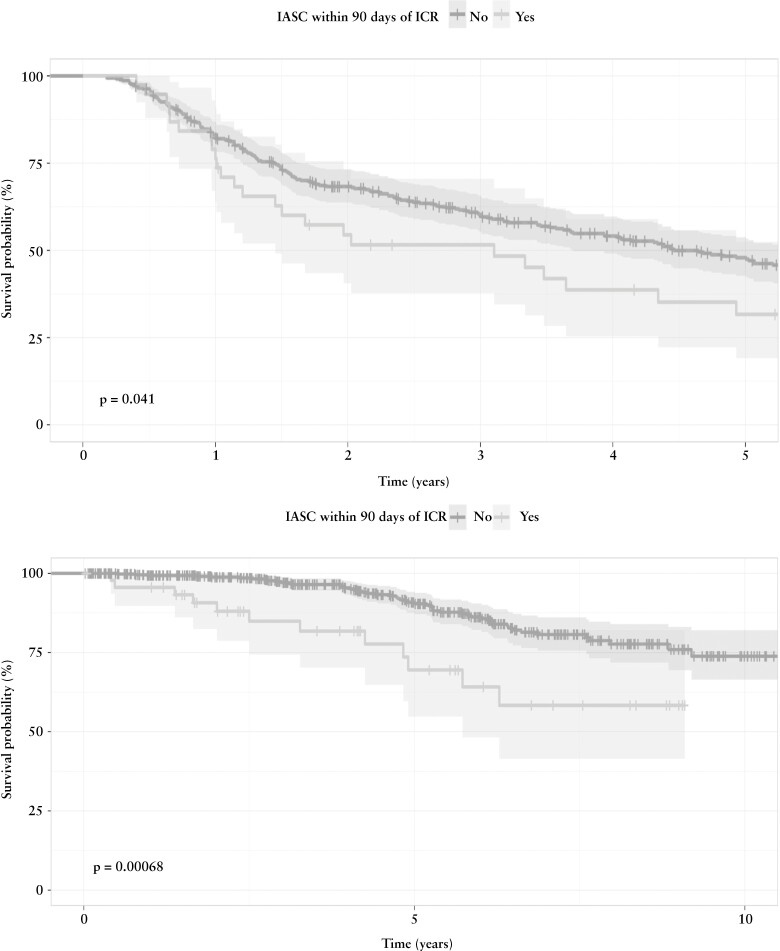
Methods: This was a retrospective study of adult Crohn's disease patients undergoing ileocolonic resection with primary anastomosis between 2009 and 2020. IASC was defined as anastomotic leak or intra-abdominal abscess within 90 days of the date of surgery. Multivariable logistic and Cox proportional hazard modelling were performed to assess the impact of IASC on endoscopic POR [modified Rutgeerts' score ≥ i2b] at index postoperative ileocolonoscopy and long-term surgical recurrence.
Results: In 535 Crohn's disease patients [median age 35 years, 22.1% active smokers, 35.7% one or more prior resection] had an ileocolonic resection with primary anastomosis. A minority of patients [N = 47; 8.8%] developed postoperative IASC. In total, 422 [78.9%] patients had one or more postoperative ileocolonoscopies, of whom 163 [38.6%] developed endoscopic POR. After adjusting for other risk factors for postoperative recurrence, postoperative IASC was associated with significantly greater odds (adjusted odds ratio [aOR]: 2.45 [1.23-4.97]; p = 0.01) and decreased time (adjusted hazards ratio [aHR]: 1.60 [1.04-2.45]; p = 0.03] to endoscopic POR. Furthermore, IASC was associated with increased risk (aOR: 2.3 [1.04-4.87] p = 0.03) and decreased survival-free time [aHR: 2.53 [1.31-4.87]; p = 0.006] for surgical recurrence.
Conclusion: IASC is associated with an increased risk for endoscopic and surgical POR of Crohn's disease. Preoperative optimization to prevent IASC, in addition to postoperative biological prophylaxis, may help reduce the risk for endoscopic and surgical POR.
Keywords: Crohn’s disease; infection; postoperative complications; postoperative recurrence.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
There are no disclosures relevant to the data presented in this paper. Professional disclosures are listed: Florian Rieder reports consulting and advisory boards for Adnovate, Agomab, Allergan, AbbVie, Boehringer-Ingelheim, Celgene/BMS, CDISC, Cowen, Galmed, Genentech, Gilead, Gossamer, Guidepoint, Helmsley, Index Pharma, Jannsen, Koutif, Mestag, Metacrine, Morphic, Organovo, Origo, Pfizer, Pliant, Prometheus Biosciences, Receptos, RedX, Roche, Samsung, Surmodics, Surrozen, Takeda, Techlab, Theravance, Thetis, UCB, Ysios and 89Bio and research funding from the NIH, Helmsley Charitable Trust, Crohn’s and Colitis Foundation, UCB, Pliant, BMS, AbbVie, Pfizer, Boehringer Ingelheim, Morphic and Kenneth Rainin Foundation. Jessica Philpott reports serving as a speaker for Abbvie. Edward Barnes reports consulting for AbbVie, Gilead, Pfizer and TARGET-RWE. Jordan Axelrad reports receiving research grants from BioFire Diagnostics; consultancy fees or honorarium from BioFire Diagnostics and Janssen; and holds U.S. patent 2012/0052124A1. Stefan Holubar reports consulting fees for Shionogi, Takeda and Guidepoint; research grant support from Crohn’s & Colitis Foundation. Amy Lightner reports serving as a consultant for Takeda. Miguel Regueiro reports serving on the advisory board or consultant for Abbvie, Janssen, UCB, Takeda, Pfizer, Miraca Labs, Amgen, Celgene, Seres, Allergan, Genentech, Gilead, Salix, Prometheus, Lilly, TARGET Pharma Solutions, ALFASIGMA, S.
Figures
Similar articles
-
Differential risk of disease progression between isolated anastomotic ulcers and mild ileal recurrence after ileocolonic resection in patients with Crohn's disease.Gastrointest Endosc. 2019 Aug;90(2):269-275. doi: 10.1016/j.gie.2019.01.029. Epub 2019 Feb 6. Gastrointest Endosc. 2019. PMID: 30738034 Free PMC article.
-
KONO-S Anastomosis Is Not Superior to Conventional Anastomosis for the Reduction of Postoperative Endoscopic Recurrence in Crohn's Disease.Inflamm Bowel Dis. 2024 Oct 3;30(10):1670-1677. doi: 10.1093/ibd/izad214. Inflamm Bowel Dis. 2024. PMID: 37776562
-
Postoperative Crohn's Disease Recurrence Risk and Optimal Biologic Timing After Temporary Diversion Following Ileocolic Resection.Inflamm Bowel Dis. 2025 Mar 3;31(3):686-695. doi: 10.1093/ibd/izae117. Inflamm Bowel Dis. 2025. PMID: 38842693
-
Risk factors and implications of anastomotic complications after surgery for Crohn's disease.World J Gastrointest Surg. 2015 Oct 27;7(10):237-42. doi: 10.4240/wjgs.v7.i10.237. World J Gastrointest Surg. 2015. PMID: 26523211 Free PMC article. Review.
-
Endoscopic Assessment of Postoperative Recurrence in Crohn's Disease: Evolving Concepts.Gastrointest Endosc Clin N Am. 2025 Jan;35(1):121-140. doi: 10.1016/j.giec.2024.04.010. Epub 2024 May 23. Gastrointest Endosc Clin N Am. 2025. PMID: 39510683 Review.
Cited by
-
Neutrophil-to-Lymphocyte Ratio as a Biomarker for Postoperative Complications in Crohn's Disease.In Vivo. 2025 May-Jun;39(3):1580-1590. doi: 10.21873/invivo.13958. In Vivo. 2025. PMID: 40295000 Free PMC article.
-
Risk factors for anastomotic complications after elective intestinal resection in Crohn's disease.Turk J Surg. 2024 Jun 28;40(2):136-144. doi: 10.47717/turkjsurg.2024.6417. eCollection 2024 Jun. Turk J Surg. 2024. PMID: 39628509 Free PMC article.
-
Anastomotic Configuration and Temporary Diverting Ileostomy Do Not Increase Risk of Anastomotic Stricture in Postoperative Crohn's Disease.Am J Gastroenterol. 2023 Dec 1;118(12):2212-2219. doi: 10.14309/ajg.0000000000002393. Epub 2023 Jul 7. Am J Gastroenterol. 2023. PMID: 37410924 Free PMC article.
-
Timing of individualized surgical intervention in Crohn's disease.World J Gastrointest Surg. 2022 Dec 27;14(12):1320-1328. doi: 10.4240/wjgs.v14.i12.1320. World J Gastrointest Surg. 2022. PMID: 36632120 Free PMC article. Review.
-
Post-operative Crohn's Disease Recurrence and Infectious Complications: A Transcriptomic Analysis.Dig Dis Sci. 2025 Jan;70(1):203-214. doi: 10.1007/s10620-024-08595-3. Epub 2024 Aug 31. Dig Dis Sci. 2025. PMID: 39215865 Free PMC article.
References
-
- Bernstein CN, Loftus EV, Ng SC, et al. . Hospitalisations and surgery in Crohn’s disease. Gut 2012;61:622–9. - PubMed
-
- Nguyen GC, Nugent Z, Shaw S, et al. . Outcomes of patients with Crohn’s disease improved from 1988 to 2008 and were associated with increased specialist care. Gastroenterology 2011;141:90–7. - PubMed
-
- Vind I, Riis L, Jess T, et al. . Increasing incidences of inflammatory bowel disease and decreasing surgery rates in Copenhagen City and County, 2003–2005: a population-based study from the Danish Crohn colitis database. Am J Gastroenterol 2006;101:1274–82. - PubMed
-
- Ramadas AV, Gunesh S, Thomas GAO, et al. Natural history of Crohn’s disease in a population-based cohort from Cardiff (1986–2003): a study of changes in medical treatment and surgical resection rates. Gut. 2010;59:1200–6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
