

Effectiveness of TNF-inhibitors, abatacept, IL6-inhibitors and JAK-inhibitors in 31 846 patients with rheumatoid arthritis in 19 registers from the 'JAK-pot' collaboration
- PMID: 35705376
- PMCID: PMC9484385
- DOI: 10.1136/annrheumdis-2022-222586
Effectiveness of TNF-inhibitors, abatacept, IL6-inhibitors and JAK-inhibitors in 31 846 patients with rheumatoid arthritis in 19 registers from the 'JAK-pot' collaboration
Erratum in
-
Correction: Effectiveness of TNF-inhibitors, abatacept, IL6-inhibitors and JAK-inhibitors in 31 846 patients with rheumatoid arthritis in 19 registers from the 'JAK-pot' collaboration.Ann Rheum Dis. 2024 Jan 2;83(1):e1. doi: 10.1136/ard-2022-222586corr1. Ann Rheum Dis. 2024. PMID: 38167602 Free PMC article. No abstract available.
Abstract
Background: JAK-inhibitors (JAKi), recently approved in rheumatoid arthritis (RA), have changed the landscape of treatment choices. We aimed to compare the effectiveness of four current second-line therapies of RA with different modes of action, since JAKi approval, in an international collaboration of 19 registers.
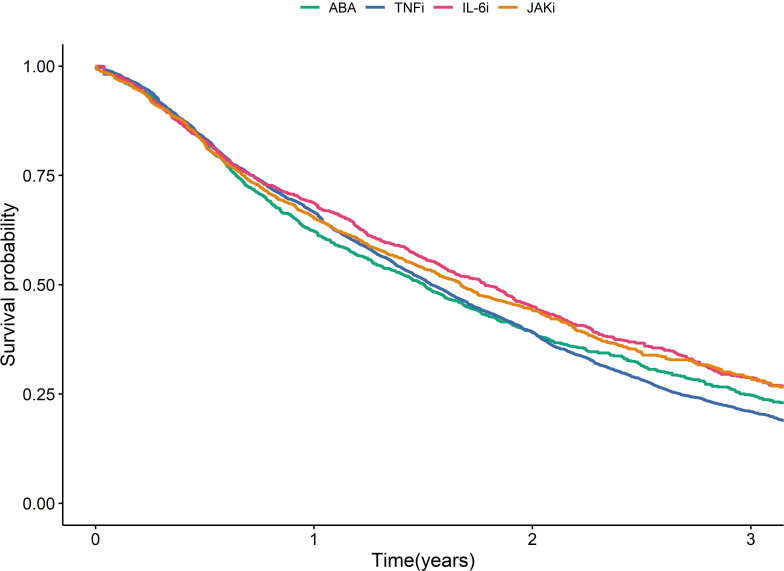
Methods: In this observational cohort study, patients initiating tumour necrosis factor inhibitors (TNFi), interleukin-6 inhibitors (IL-6i), abatacept (ABA) or JAKi were included. We compared the effectiveness of these treatments in terms of drug discontinuation and Clinical Disease Activity Index (CDAI) response rates at 1 year. Analyses were adjusted for patient, disease and treatment characteristics, including lines of therapy and accounted for competing risk.
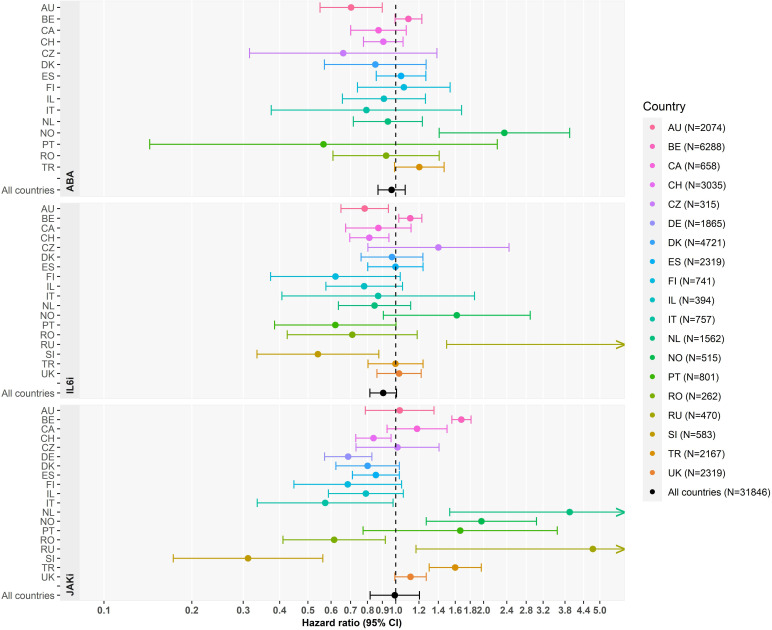
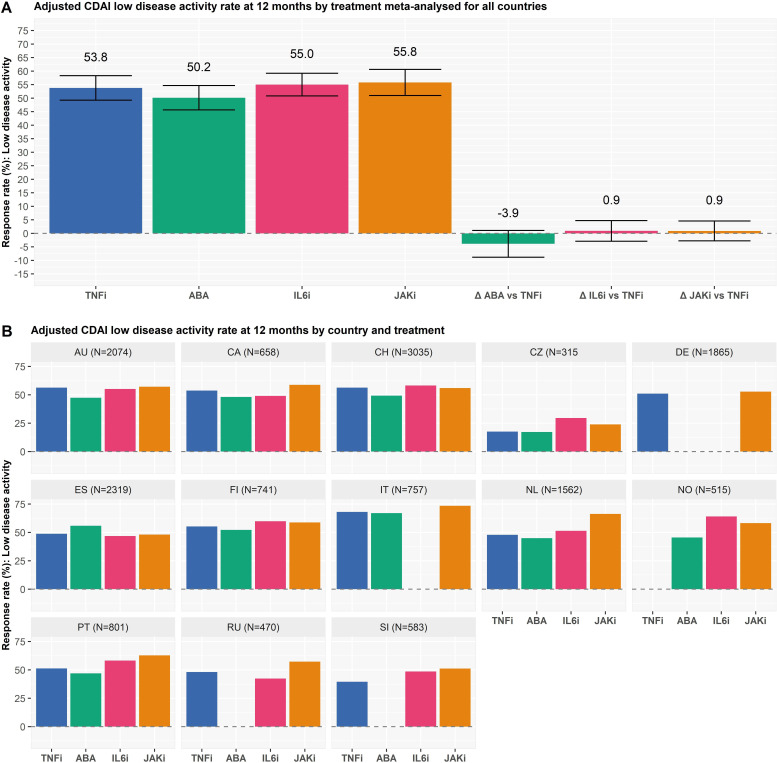
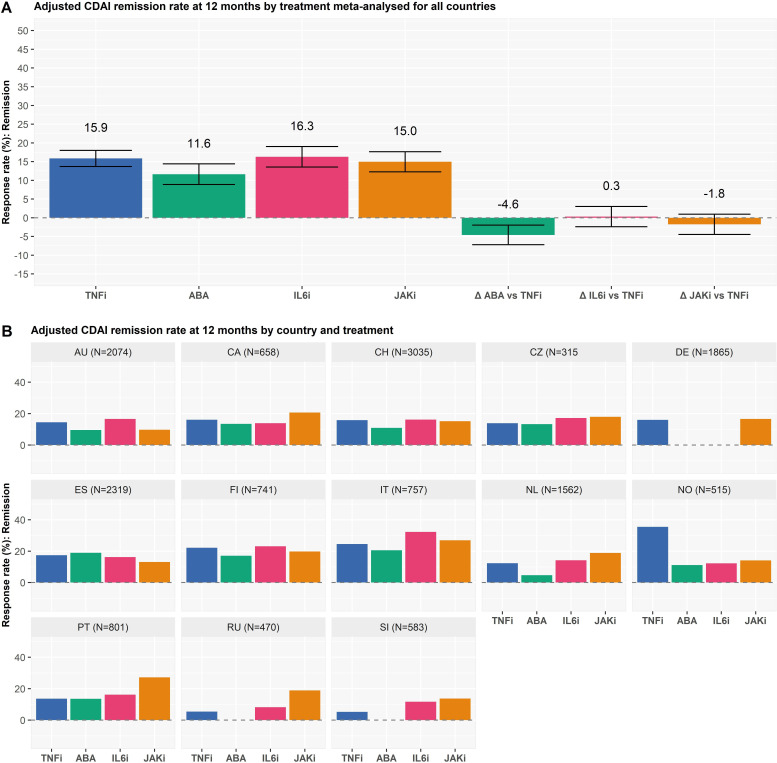
Results: We included 31 846 treatment courses: 17 522 TNFi, 2775 ABA, 3863 IL-6i and 7686 JAKi. Adjusted analyses of overall discontinuation were similar across all treatments. The main single reason of stopping treatment was ineffectiveness. Compared with TNFi, JAKi were less often discontinued for ineffectiveness (adjusted HR (aHR) 0.75, 95% CI 0.67 to 0.83), as was IL-6i (aHR 0.76, 95% CI 0.67 to 0.85) and more often for adverse events (aHR 1.16, 95% CI 1.03 to 1.33). Adjusted CDAI response rates at 1 year were similar between TNFi, JAKi and IL-6i and slightly lower for ABA.
Conclusion: The adjusted overall drug discontinuation and 1 year response rates of JAKi and IL-6i were similar to those observed with TNFi. Compared with TNFi, JAKi were more often discontinued for adverse events and less for ineffectiveness, as were IL-6i.
Keywords: Arthritis, Rheumatoid; Biological Therapy; Epidemiology; Therapeutics; Tumor Necrosis Factor Inhibitors.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KL reports personal fees from Gilead-Galapagos, Pfizer, Viatris, Celltrion, outside the submitted work. ML reports speaking fee from Boehringer Inghelheim, outside the submitted work. DM has nothing to disclose. SAB report grants from Pfizer, outside the submitted work. DC report grants, personal fees and non-financial support from Abbvie, grants, personal fees and non-financial support from Amgen, grants, personal fees and non-financial support from BMS, grants, personal fees and non-financial support from Eli Lilly, grants, personal fees and non-financial support from Merck, grants, personal fees and non-financial support from Novartis, grants, personal fees and non-financial support from Pfizer, grants, personal fees and non-financial support from Roche, grants, personal fees and non-financial support from Sanofi-Genzyme, grants, personal fees and non-financial support from UCB, grants, personal fees and non-financial support from Sandoz, outside the submitted work. CC reports personal fees from Abbvie, Amgen, Boehringer Ingelheim, Ewopharma, Lilly, Novartis, Pfizer outside the submitted work. RC has nothing to disclose. DDC has nothing to disclose. LD reports institutional grant from BMS outside the present work and speakers bureau from Eli Lilly and Galderma. OE has nothing to disclose. E-MH reports personal fees from AbbVie, Sanofi, Sobi ; institutional grants from Novo Nordic Foundation, Danish Rheumatism Association, Danish Regions Medicine Grants, Roche, Novartis, AbbVie outside the submitted work. DH has nothing to discloseKLH reports honoraria from Abbvie and grants from Pfizer and BMS outside the submitted work, and is supported by the NIHR Manchester Biomedical Research Centre. FI reports speaking fees from Abbvie, BMS, Eli-Lilly, Roche, MSD, Galapagos, Pfizer, Celltrion, Janssen outside the submitted work. NI reports grants from Roche, Pfizer, personal fees from AbbVie, Roche, Pfizer, UCB, Novartis,Amgen, Lilly, MSD. LK-F has nothing to disclose. EKK has nothing to disclose. TKK reports fees for speaking and/or consulting last 2 years from AbbVie, Amgen, Celltrion, Egis, Evapharma, Ewopharma, Gilead, Hikma, Janssen, Mylan, Novartis, Oktal, Pfizer, Sandoz, UCB. BFL reports personal fees from Abbvie, personal fees from Biogen, personal fees from Celgene, personal fees from Eli Lilly, personal fees from MSD, personal fees from Pfizer, personal fees from Roche, and personal fees from Novartis and Sandoz. GL reports personal fees from Abbvie, personal fees from Eli Lilly, personal fees from MSD, personal fees from Novartis, personal fees from Pfizer, personal fees from Roche, personal fees from Janssen, personal fees from BMS, outside the submitted work. DCN reports grants from Roche, during the conduct of the study; personal fees from Abbvie, personal fees from BMS, grants from Celgene, personal fees from Lilly, grant from MSD, personal fees from Novartis, personal fees from Pfizer, personal fees from UCB, outside the submitted work. KP has received honoraria for lectures and consultations from: AbbVie, BMS, Egis, Roche, Amgen, MSD, Medac, Eli Lilly, Pfizer. MPS reports personal fees from Janssen, MSD, Sanofi, outside the submitted work. ZR honoraria for lectures and consultations from: Abbvie, Pfizer, MSD, Medis, Roche, outside the submitted work. MJS reports personal fees from AbbVie, personal fees from Pfizer, personal fees from Novartis, personal fees from Roche, outside the submitted work. AS reports speaker honoraria from AbbVie, BMS, MSD, Pfizer, and Roche. PV reports speakers bureau for Eli Lilly, MSD, Galapagos, Roularta, consultancy fees from Galapagos, Gilead, Pfizer, Sanofi, Sidekick Health, Eli Lilly, Nordic Pharma, ABBVIE, Celltrion, BMS, UCB and is the grant holder from the Pfizer Chair Management of Early Rheumatoid Arthritis at KU Leuven. DSC has nothing to disclose. AF reports grants from AbbVie, BMS, Eli-Lilly, Galapagos and Pfizer and speaker honoraria (educational events or symposia) from companies producing several of the targeted therapies that are included in this analysis (honoraria < 10’000 USD): AbbVie, BMS, Eli-Lilly, Gilead, MSD, Pfizer. Clinical work in Czech Republic was partially supported by the project from the Ministry of Health for conceptual development of research organisation MZ00023728023728 (Institute of Rheumatology). BIOBADASER has received funding from Fundacion Española de Reumatología, the Spanish Medicines and Health Products Agency (Agencia Española del Medicamento y Productos Sanitarios) and equal grants from pharmaceutical companies (AbbVie, BMS, Celltrion, Galapagos, Janssen, Lilly, MSD, Novartis, Pfizer, Regeneron, Roche, Samsung, Schering‐Plough and UCB). BioRx.si has received funding for clinical research paid to Društvo za razvoj revmatologije from AbbVie, Roche, Medis, MSD, Biogen, Amgen, Sanofi, Celgene and Pfizer. The British Society for Rheumatology Biologics Register in Rheumatoid Arthritis (BSRBR-RA) is funded by a grant from the British Society for Rheumatology (BSR). The BSR currently receives funding from Abbvie, Amgen, Celltrion HC, Eli Lilly, Pfizer, Samsung Bioepis, Sanofi, Sandoz and in the past Hospira, MSD, Roche, SOBI and UCB. This income finances a wholly separate contract between the BSR and The University of Manchester to host the BSRBR-RA. All decisions concerning study design, data capture, analyses, interpretation and publication are made autonomously of any industrial contribution. The BSRBR-RA would like to gratefully acknowledge the support of the National Institute for Health Research, through the Local Clinical Research Networks in England (and equivalent organisations in the devolved nations) at participating centres and the BSRBR-RA Control Centre Consortium. DANBIO was partially supported by public and private funding (AbbVie, Biogen, Bristol Myers Squibb, Eli Lilly, MSD, Novartis, Pfizer, Roche, Sanofi, UCB). NOR-DMARD was has been supported with research funding to Diakonhjemmet Hospital from AbbVie, Amgen, BMS, MSD, Novartis, Pfizer and UCB. The RABBIT register is currently supported by an unconditional grant with equal parts from AbbVie, Amgen, BMS, Celltrion, Fresenius Kabi, Galapagos, Hexal, Lilly, MSD, Viatris, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis, and UCB. REUMA. PT is supported by unrestricted grants from Abbvie, Biogen, Celgene, MSD, Roche, Sanofi and Pfizer. ROB-FIN is funded by AbbVie, Hospira, BMS, MSD, Pfizer, Roche and UCB. The Romanian Registry of Rheumatic Diseases (RRBR) uses unrestricted grants from AbbVie, Pfizer, Eli Lilly, Ewopharma, Nopvartis MSD, Roche, UCB, and BMS. Swiss Clinical Quality Management in Rheumatic Diseases (SCQM) database is sponsored by public and industrial support (http://scqm.ch/en/sponsoren/).
Figures
References
-
- Maini R, St Clair EW, Breedveld F, et al. Infliximab (chimeric anti-tumour necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomised phase III trial. attract Study Group. Lancet 1999;354:1932–9. 10.1016/S0140-6736(99)05246-0 - DOI - PubMed
-
- Keystone E, Heijde Dvander, Mason D, et al. Certolizumab pegol plus methotrexate is significantly more effective than placebo plus methotrexate in active rheumatoid arthritis: findings of a fifty-two-week, phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum 2008;58:3319–29. 10.1002/art.23964 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
