

Prospective intraoperative and histologic evaluation of cavernous sinus medial wall invasion by pituitary adenomas and its implications for acromegaly remission outcomes
- PMID: 35705579
- PMCID: PMC9200976
- DOI: 10.1038/s41598-022-12980-1
Prospective intraoperative and histologic evaluation of cavernous sinus medial wall invasion by pituitary adenomas and its implications for acromegaly remission outcomes
Abstract
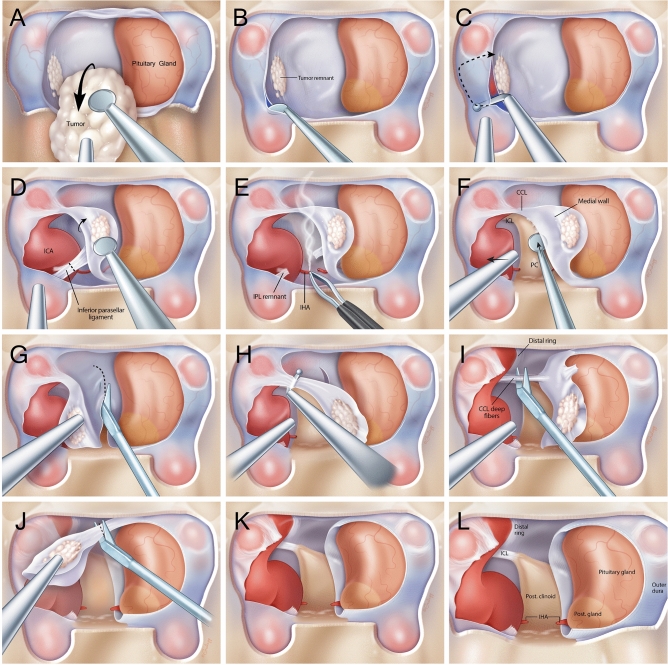
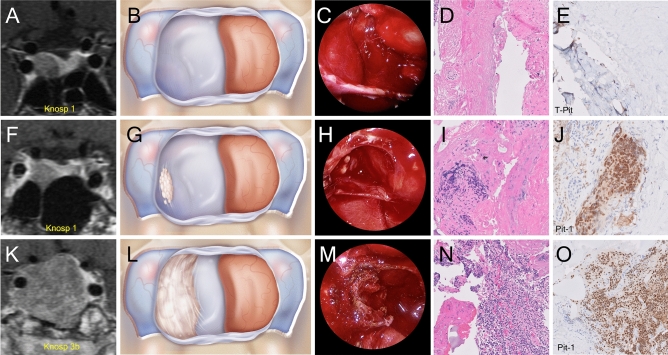
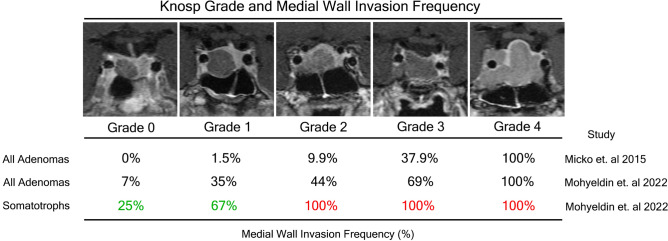
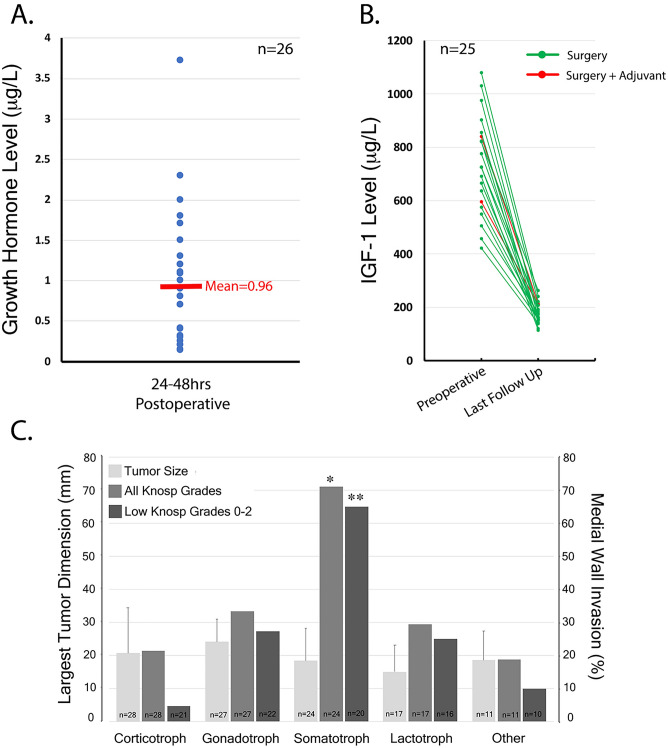
Recurrence and biochemical remission rates vary widely among different histological subtypes of pituitary adenoma. In this prospective study, we evaluated 107 consecutive primary pituitary adenomas operated on by a single neurosurgeon including 28 corticotroph, 27 gonadotroph, 24 somatotroph, 17 lactotroph, 5 null-cell and 6 plurihormonal. In each case, we performed direct endoscopic intraoperative inspection of the medial wall of the cavernous sinus, which was surgically removed when invasion was visualized. This was performed irrespective of tumor functional status. Medial wall resection was performed in 47% of pituitary adenomas, and 39/50 walls confirmed pathologic evidence of invasion, rendering a positive predictive value of intraoperative evaluation of medial wall invasion of 78%. We show for the first-time dramatic disparities in the frequency of medial wall invasion among pathological subtypes. Somatotroph tumors invaded the medial wall much more often than other adenoma subtypes, 81% intraoperatively and 69% histologically, followed by plurihormonal tumors (40%) and gonadotroph cell tumors (33%), both with intraoperative positive predictive value of 100%. The least likely to invade were corticotroph adenomas, at a rate of 32% intraoperatively and 21% histologically, and null-cell adenomas at 0%. Removal of the cavernous sinus medial wall was not associated with permanent cranial nerve morbidity nor carotid artery injury, although 4 patients (all Knosp 3-4) experienced transient diplopia. Medial wall resection in acromegaly resulted in the highest potential for biochemical remission ever reported, with an average postoperative day 1 GH levels of 0.96 ug/L and surgical remission rates of 92% based on normalization of IGF-1 levels after surgery (mean = 15.56 months; range 3-30 months). Our findings suggest that tumor invasion of the medial wall of the cavernous sinus may explain the relatively low biochemical remission rates currently seen for acromegaly and illustrate the relevance of advanced intradural surgical approaches for successful and durable outcomes in endonasal pituitary surgery for functional adenomas.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- WHO classification of tumours of endocrine organs, 4th edn. Lyon, France: IARC Press 2017.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
