

A new method to quantify left ventricular mass by 2D echocardiography
- PMID: 35705586
- PMCID: PMC9200734
- DOI: 10.1038/s41598-022-13677-1
A new method to quantify left ventricular mass by 2D echocardiography
Abstract
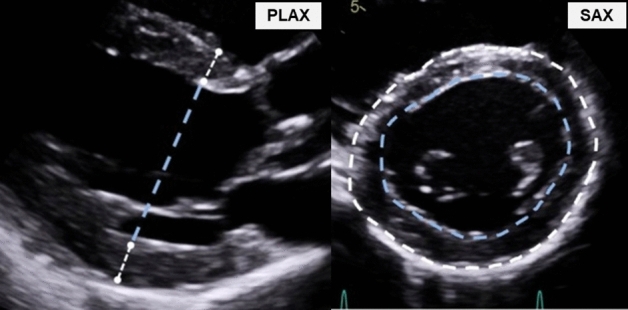
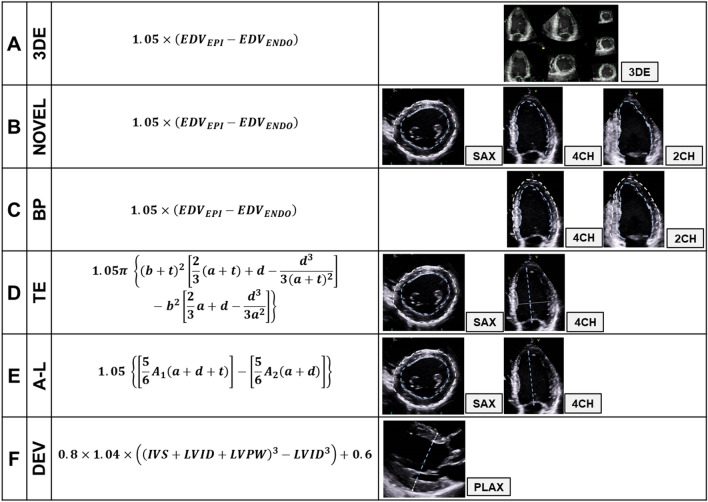
Increased left ventricular mass (LVM) is a strong independent predictor for adverse cardiovascular events, but conventional echocardiographic methods are limited by poor reproducibility and accuracy. We developed a novel method based on adding the mean wall thickness from the parasternal short axis view, to the left ventricular end-diastolic volume acquired using the biplane model of discs. The participants (n = 85) had various left ventricular geometries and were assessed using echocardiography followed immediately by cardiac magnetic resonance, as reference. We compared our novel two-dimensional (2D) method to various conventional one-dimensional (1D) and other 2D methods as well as the three-dimensional (3D) method. Our novel method had better reproducibility in intra-examiner [coefficients of variation (CV) 9% vs. 11-14%] and inter-examiner analysis (CV 9% vs. 10-20%). Accuracy was similar to the 3D method (mean difference ± 95% limits of agreement, CV): Novel: 2 ± 50 g, 15% vs. 3D: 2 ± 51 g, 16%; and better than the "linear" 1D method by Devereux (7 ± 76 g, 23%). Our novel method is simple, has considerable better reproducibility and accuracy than conventional "linear" 1D methods, and similar accuracy as the 3D-method. As the biplane model forms part of the standard echocardiographic protocol, it does not require specific training and provides a supplement to the modern echocardiographic report.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
