

Vectorcardiography-derived index allows a robust quantification of ventricular electrical synchrony
- PMID: 35705598
- PMCID: PMC9200867
- DOI: 10.1038/s41598-022-14000-8
Vectorcardiography-derived index allows a robust quantification of ventricular electrical synchrony
Abstract
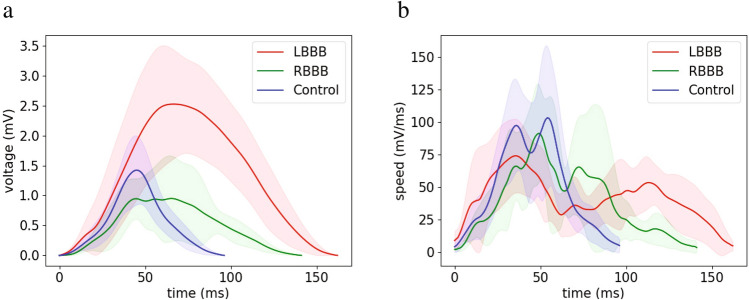
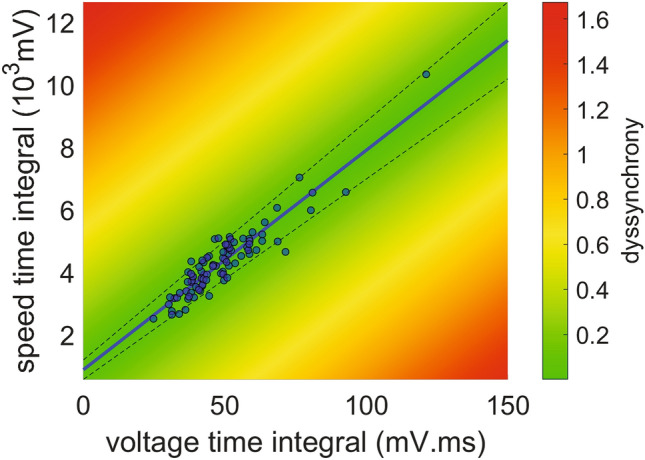
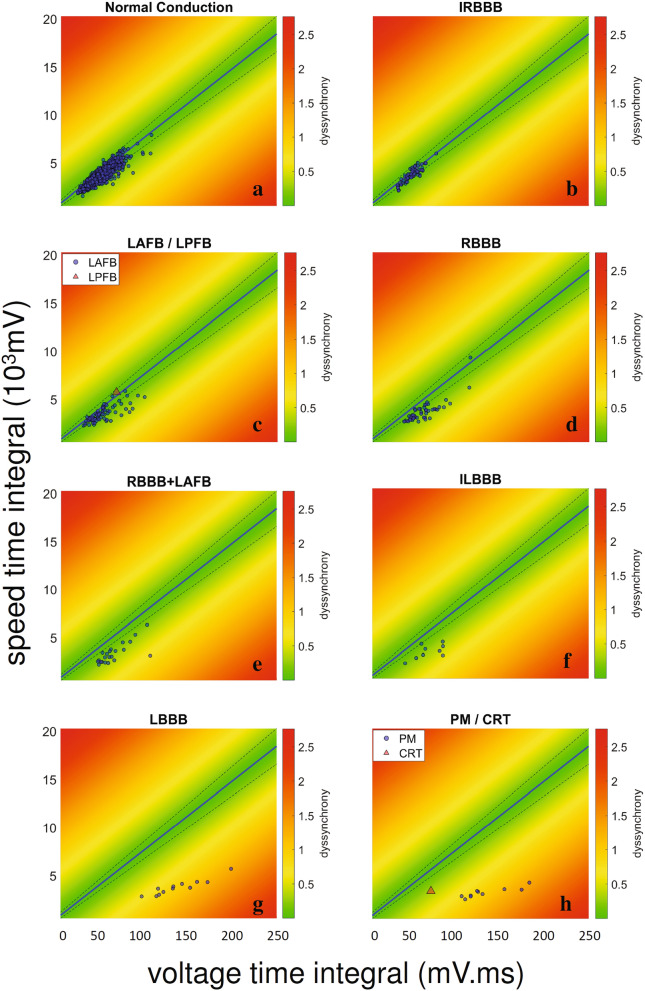
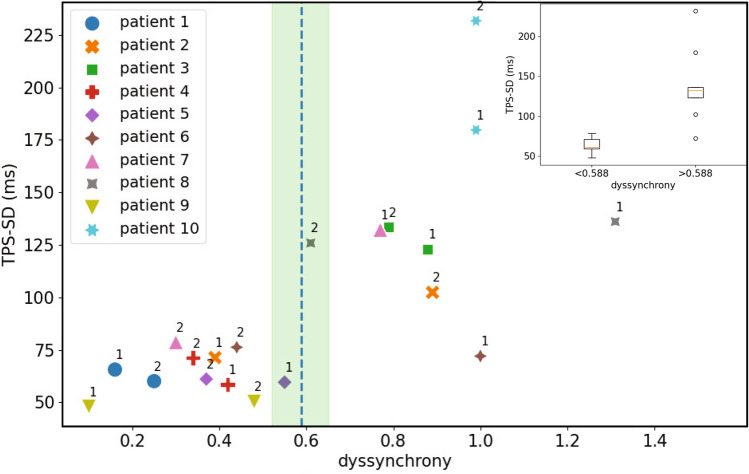
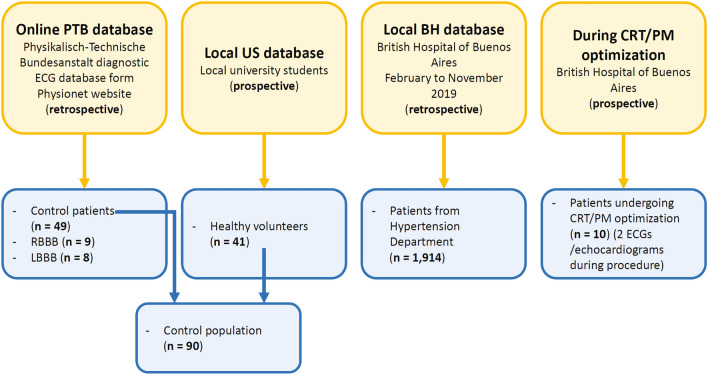
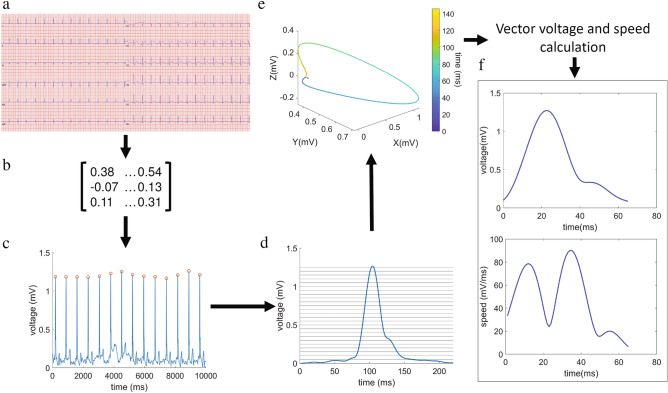
Alteration of muscle activation sequence is a key mechanism in heart failure with reduced ejection fraction. Successful cardiac resynchronization therapy (CRT), which has become standard therapy in these patients, is limited by the lack of precise dyssynchrony quantification. We implemented a computational pipeline that allows assessment of ventricular dyssynchrony by vectorcardiogram reconstruction from the patient's electrocardiogram. We defined a ventricular dyssynchrony index as the distance between the voltage and speed time integrals of an individual observation and the linear fit of these variables obtained from a healthy population. The pipeline was tested in a 1914-patient population. The dyssynchrony index showed minimum values in heathy controls and maximum values in patients with left bundle branch block (LBBB) or with a pacemaker (PM). We established a critical dyssynchrony index value that discriminates electrical dyssynchronous patterns (LBBB and PM) from ventricular synchrony. In 10 patients with PM or CRT devices, dyssynchrony indexes above the critical value were associated with high time to peak strain standard deviation, an echocardiographic measure of mechanical dyssynchrony. Our index proves to be a promising tool to evaluate ventricular activation dyssynchrony, potentially enhancing the selection of candidates for CRT, device configuration during implantation, and post-implant optimization.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
