

HOPS-R01 phase II trial evaluating neoadjuvant S-1 therapy for resectable pancreatic adenocarcinoma
- PMID: 35705607
- PMCID: PMC9200853
- DOI: 10.1038/s41598-022-14094-0
HOPS-R01 phase II trial evaluating neoadjuvant S-1 therapy for resectable pancreatic adenocarcinoma
Abstract
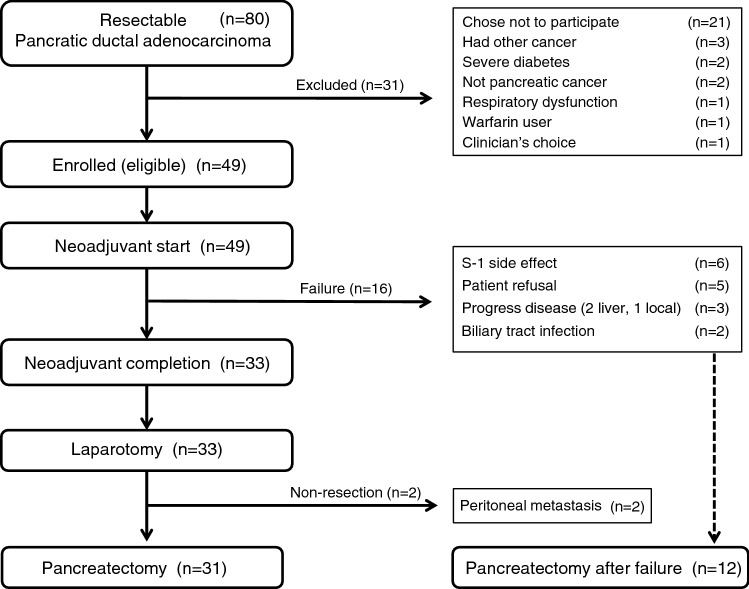
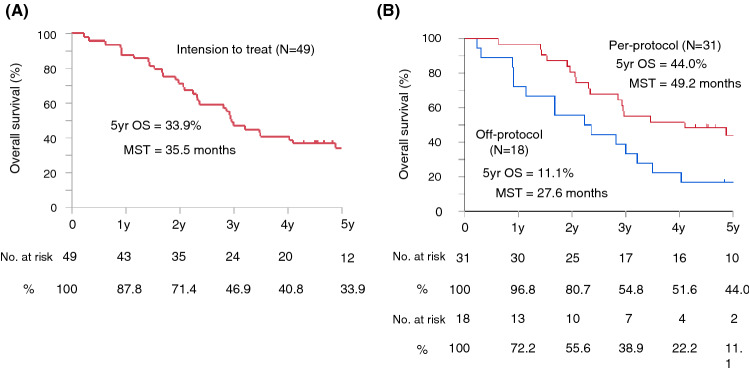
Although neoadjuvant therapy (Nac) is recommended for high-risk resectable pancreatic cancer (R-PDAC), evidence regarding specific regimes is scarce. This report aimed to investigate the efficacy of S-1 Nac for R-PDAC. In a multicenter phase II trial, we investigated the efficacy of Nac S-1 (an oral fluoropyrimidine agent containing tegafur, gimeracil, and oteracil potassium) in R-PDAC patients. The protocol involved two cycles of preoperative S-1 chemotherapy, followed by surgery, and four cycles of postoperative S-1 chemotherapy. Two-year progression-free survival (PFS) rates were the primary endpoint. Overall survival (OS) rates and median survival time (MST) were secondary endpoints. Forty-nine patients were eligible, and 31 patients underwent resection following Nac, as per protocol (31/49; 63.3%). Per-protocol analysis included data from 31 patients, yielding the 2-year PFS rate of 58.1%, and 2-, 3-, and 5-year OS rates of 96.8%, 54.8%, and 44.0%, respectively. MST was 49.2 months. Intention-to-treat analysis involved 49 patients, yielding the 2-year PFS rate of 40.8%, and the 2-, 3-, and 5-year OS rates of 87.8%, 46.9%, and 33.9%, respectively. MST was 35.5 months. S-1 single regimen might be an option for Nac in R-PDAC; however, the high drop-out rate (36.7%) was a limitation of this study.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- National Comprehensive Cancer Network (2019) NCCN Clinical Practice Guidelines in Oncology Pancreatic Adenocarcinoma, version 3. https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf.7. Accessed July 2, 2019.
-
- Unno M, Hata T, Motoi F. Long-term outcome following neoadjuvant therapy for resectable and borderline resectable pancreatic cancer compared to upfront surgery: a meta-analysis of comparative studies by intention-to-treat analysis. Surg. Today. 2019;49:295–299. doi: 10.1007/s00595-019-01786-w. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
