

Neighborhood social cohesion and serious psychological distress among Asian, Black, Hispanic/Latinx, and White adults in the United States: a cross-sectional study
- PMID: 35705933
- PMCID: PMC9199195
- DOI: 10.1186/s12889-022-13572-4
Neighborhood social cohesion and serious psychological distress among Asian, Black, Hispanic/Latinx, and White adults in the United States: a cross-sectional study
Abstract
Background: Serious psychological distress (SPD) is common and more prevalent in women, older adults, and individuals with a low-income. Prior studies have highlighted the role of low neighborhood social cohesion (nSC) in potentially contributing to SPD; however, few have investigated this association in a large, nationally representative sample of the United States. Therefore, our objective was to investigate the overall and racial/ethnic-, sex/gender-, self-rated health status-, age-, and household income-specific relationships between nSC and SPD.
Methods: We used data from survey years 2013 to 2018 of the National Health Interview Survey to investigate nSC and SPD among Asian, Non-Hispanic (NH)-Black, Hispanic/Latinx, and NH-White men as well as women in the United States (N = 168,573) and to determine modification by race/ethnicity, sex/gender, self-rated health status, age, and annual household income. nSC was measured by asking participants four questions related to the trustworthiness and dependability of their neighbors. nSC scores were trichotomized into low (< 12), medium (12-14), and high (15-16). SPD was measured using the Kessler 6 psychological distress scale with scores ≥ 13 indicating SPD. After adjusting for sociodemographic, health behavior, and clinical confounders, we used Poisson regression with robust variance to estimate prevalence ratios (PRs) and 95% confidence intervals (CIs).
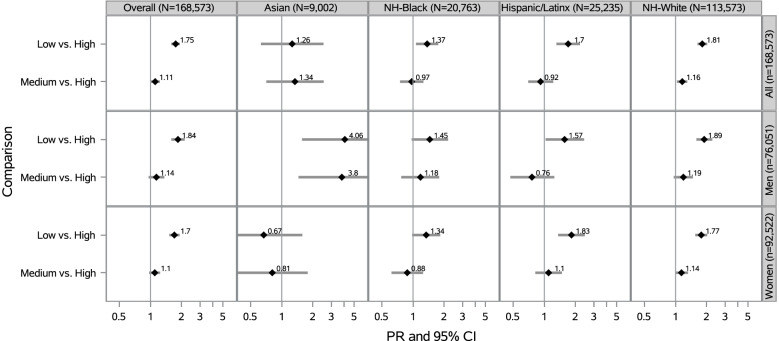
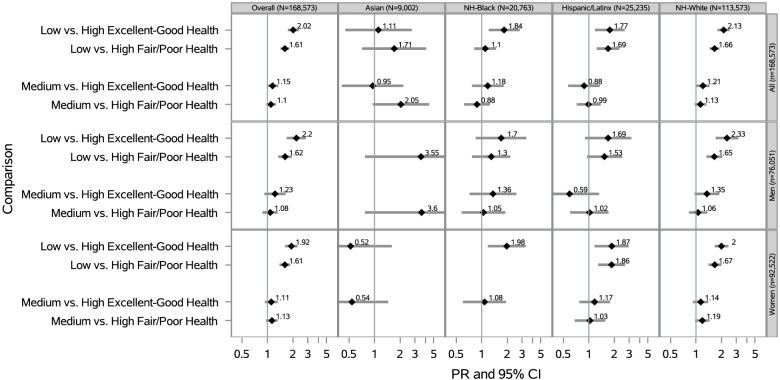
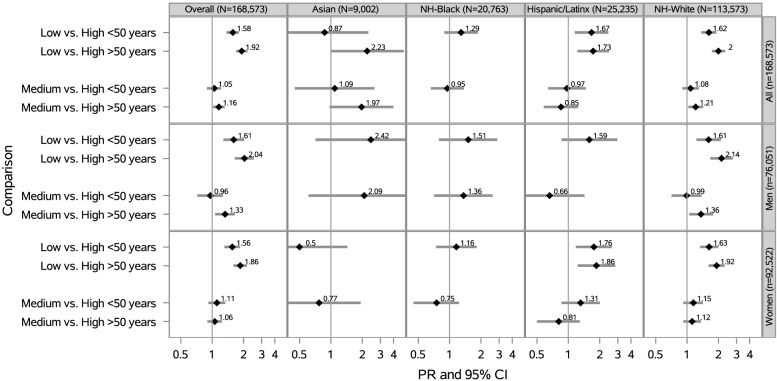
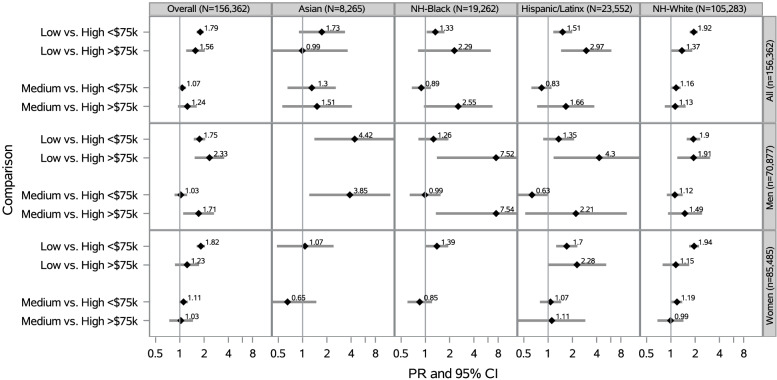
Results: Among 168,573 participants, most were Non-Hispanic (NH)-White (69%), and mean age was 47 ± 0.01 years. After adjustment, low vs. high nSC was associated with a 75% higher prevalence of SPD overall (PR = 1.75 [1.59-1.92]), 4 times the prevalence of SPD among Asian men (PR = 4.06 [1.57-10.50]), 2 times the prevalence of SPD among participants in at least good health (PR = 2.02 [95% CI: 1.74-2.35]), 92% higher prevalence of SPD among participants ≥ 50 years old (PR = 1.92 [1.70-2.18]), and approximately 3 times the prevalence of SPD among Hispanic/Latinx participants with household incomes ≥ $75,000 (PR = 2.97 [1.45-6.08]).
Conclusions: Low nSC was associated with higher SPD in the overall population and the magnitude of the association was higher in Asian men, participants who reported good health, older participants, and Hispanic/Latinx adults with higher household incomes. Future research should continue to examine how neighborhood contexts can affect health across various sociodemographic groups, especially among groups with multiple marginalized social identities.
Keywords: Community support; Economic status; Mental health; Psychological distress; Race factors; Residence characteristics.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Weissman J, Pratt LA, Miller EA, Parker JD. Serious Psychological Distress Among Adults: United States, 2009–2013. 2015. - PubMed
-
- Forman-Hoffman , , , , VL, Muhuri PK, Novak SP, Pemberton MR, Ault KL, Mannix D. The CBHSQ Report. Rockville, MD: Rockville, MD; 2014. Psychological Distress and Mortality among Adults in the U.S. Household Population.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
