

Transnasal Endoscopic and Transoral Approaches in the Biopsies of Ventral Atlas and Axis Vertebrae: A Comprehensive Retrospective Study for Preprocedural Scheme, Biopsy Procedure, Core Technique Analysis, Diagnostic Yield and Clinical Outcome
- PMID: 35706342
- PMCID: PMC9363750
- DOI: 10.1111/os.13366
Transnasal Endoscopic and Transoral Approaches in the Biopsies of Ventral Atlas and Axis Vertebrae: A Comprehensive Retrospective Study for Preprocedural Scheme, Biopsy Procedure, Core Technique Analysis, Diagnostic Yield and Clinical Outcome
Abstract
Objective: This study aims to describe and analyze the transoral and transnasal approaches for pathologies of the ventral atlas and axis vertebrae, which are considered technically challenging regions for diagnostic biopsy.
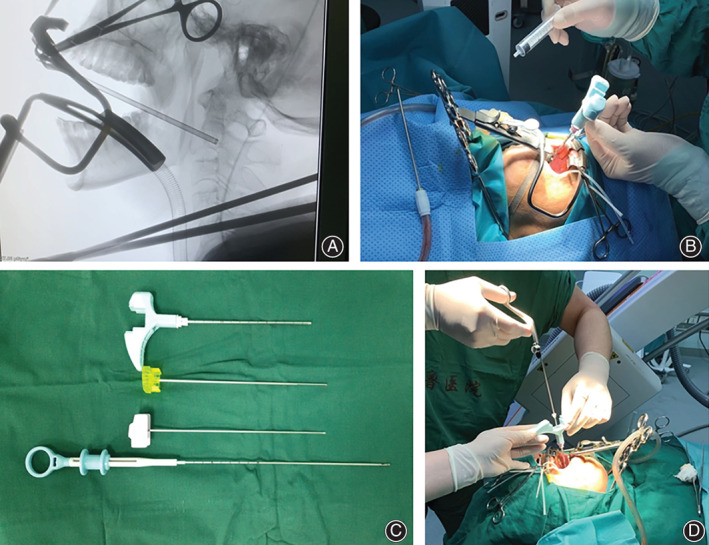
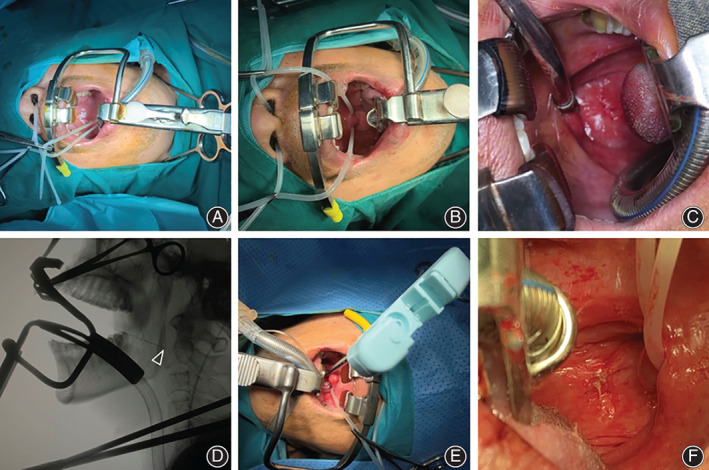
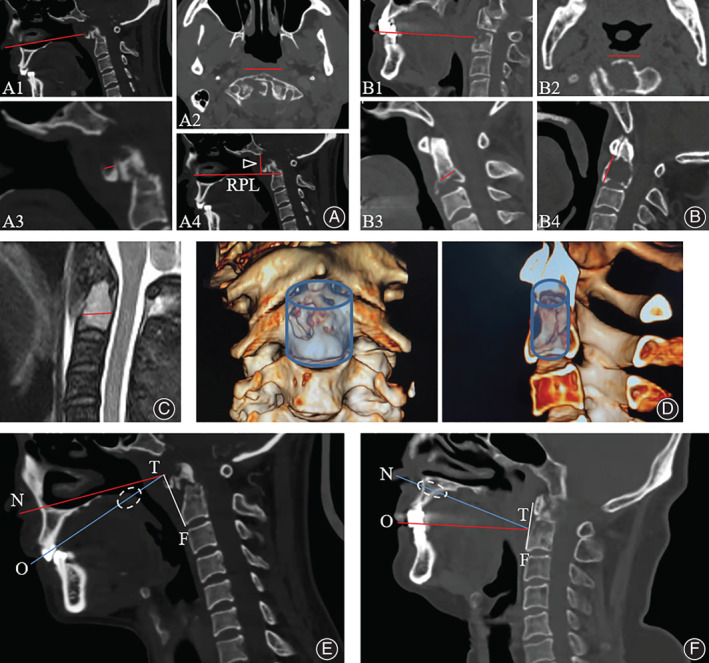
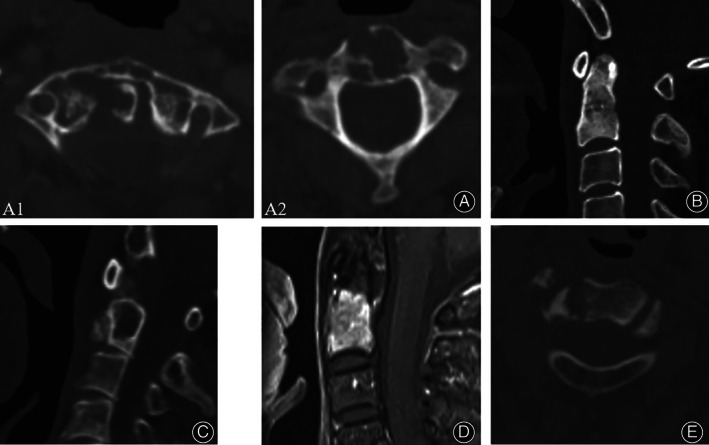
Methods: A series of transnasal endoscopic approach (TNA) and transoral approach (TOA) biopsies for the pathologies of the first and second cervical vertebrae were conducted and retrospectively analyzed from July 2014 to May 2021. The depth of the biopsy trajectory was measured on computed tomography images for all nine patients (eight males and one female with an average age of 58.11 ± 11.60 years), as were the coronal, sagittal, and vertical biopsy safe ranges. The characteristics of each lesion, including radiographic features, blood supply, and destruction of anterior or posterior vertebral body edges, were evaluated to guide the biopsy. Four biopsy core techniques (BCTs), including "lesion perforating", "aspiration", "cutting-and-scraping" and "biopsy forceps utilization" were elaborated in this study. The biopsy procedures and periprocedural precautions were demonstrated. Patient demographics, clinical data, lesion characteristics, diagnostic yield, and complications were recorded for each case.
Results: Eight TOA biopsies for the axis vertebral body and one TNA biopsy for the atlas anterior arch were successfully performed and yielded adequate pathologies. All biopsies were organized based on the preprocedural radiographic measurements, which showed that the average length of biopsy trajectory and coronal, sagittal, and vertical safe biopsy ranges were 85.00 ± 5.88, 20.63 ± 4.75, 16.25 ± 1.49, and 24.63 ± 2.26 mm, respectively, and these corresponding data were 95, 36, 9, and 26 mm in the TNA patient. Six osteolytic lesions (66.7%), one osteoblastic lesion (11.1%), and two mixed lesions (22.2%) were observed, among which seven lesions had a rich blood supply. Biopsy forceps and core needles were utilized to obtain samples in six and three patients, respectively. All the TNA and TOA biopsies were performed with cooperative application of multiple BCTs under compound anatomic and stereotactic navigations. Intraprocedural or postprocedural complications occurred in no patients who underwent the biopsy in the follow-up period (1-39 months). No significant differences were found between the preprocedural and postprocedural blood indexes and visual analogue scale scores.
Conclusion: With a sophisticated preprocedural arrangement, cooperative application of BCTs, and careful periprocedural precautions, transnasal endoscopic and transoral biopsies are two feasible, efficient, and well-tolerated procedures that achieve satisfactory diagnostic yield, complication rate, and clinical outcome.
Keywords: Atlas vertebra; Axis vertebra; Biopsy; Diagnostic yield; Transnasal approach; Transoral approach.
© 2022 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Figures
References
-
- Rehm J, Veith S, Akbar M, Kauczor HU, Weber MA. CT‐guided percutaneous spine biopsy in suspected infection or malignancy: a study of 214 patients. Rofo. 2016;188(12):1156–62. - PubMed
-
- Jeszenszky DJ, Haschtmann D, Pröbst O, Kleinstück FS, Heyde CE, Fekete TF. Tumors and metastases of the upper cervical spine (C0‐2). A special challenge. Orthopade. 2013;42(9):746–54. - PubMed
-
- Zuckerman SL, Kreines F, Powers A. Stabilization of tumor‐associated craniovertebral junction instability: indications, operative variables, and outcomes. Neurosurgery. 2017;81(2):251–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
