

Microenvironmental Landscape of Human Melanoma Brain Metastases in Response to Immune Checkpoint Inhibition
- PMID: 35706413
- PMCID: PMC10201927
- DOI: 10.1158/2326-6066.CIR-21-0870
Microenvironmental Landscape of Human Melanoma Brain Metastases in Response to Immune Checkpoint Inhibition
Abstract
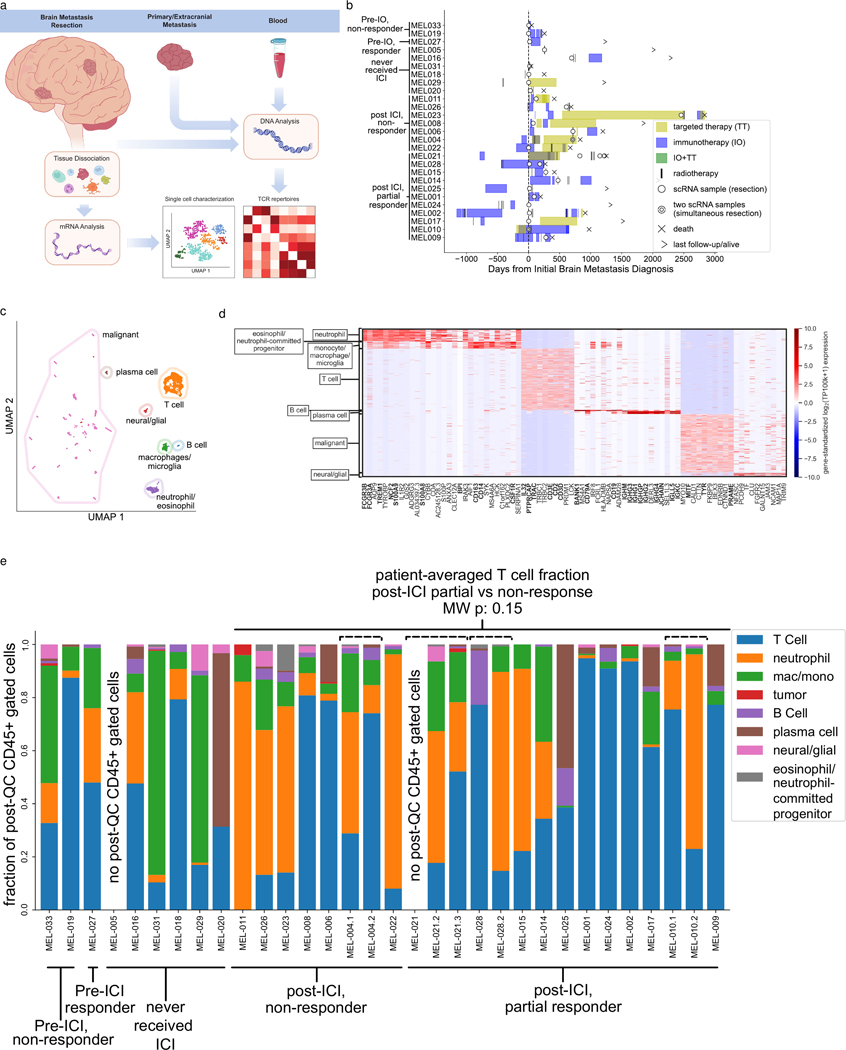
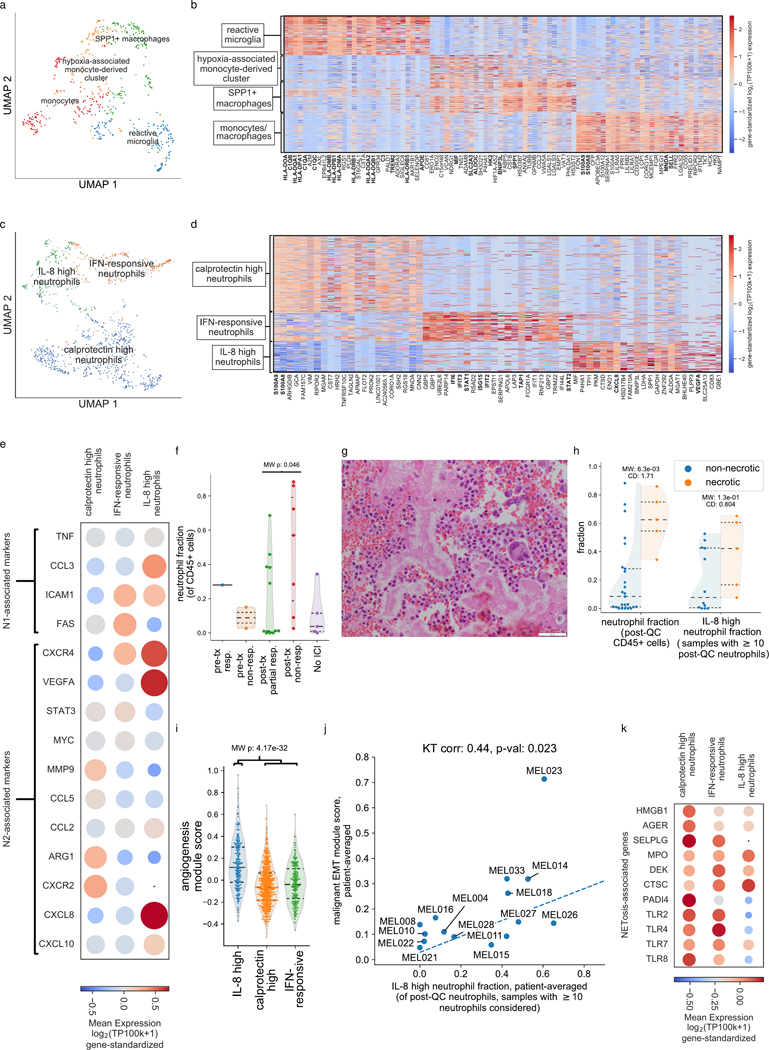
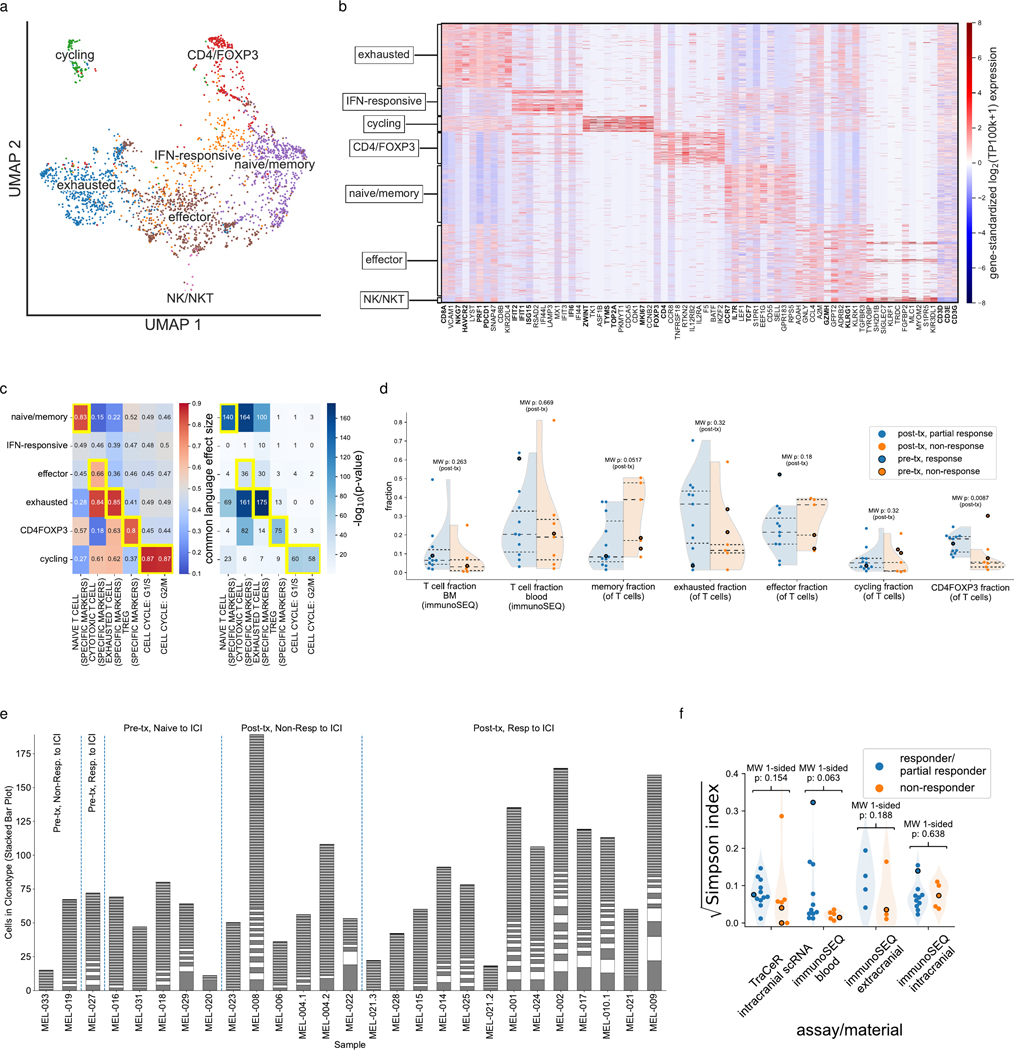
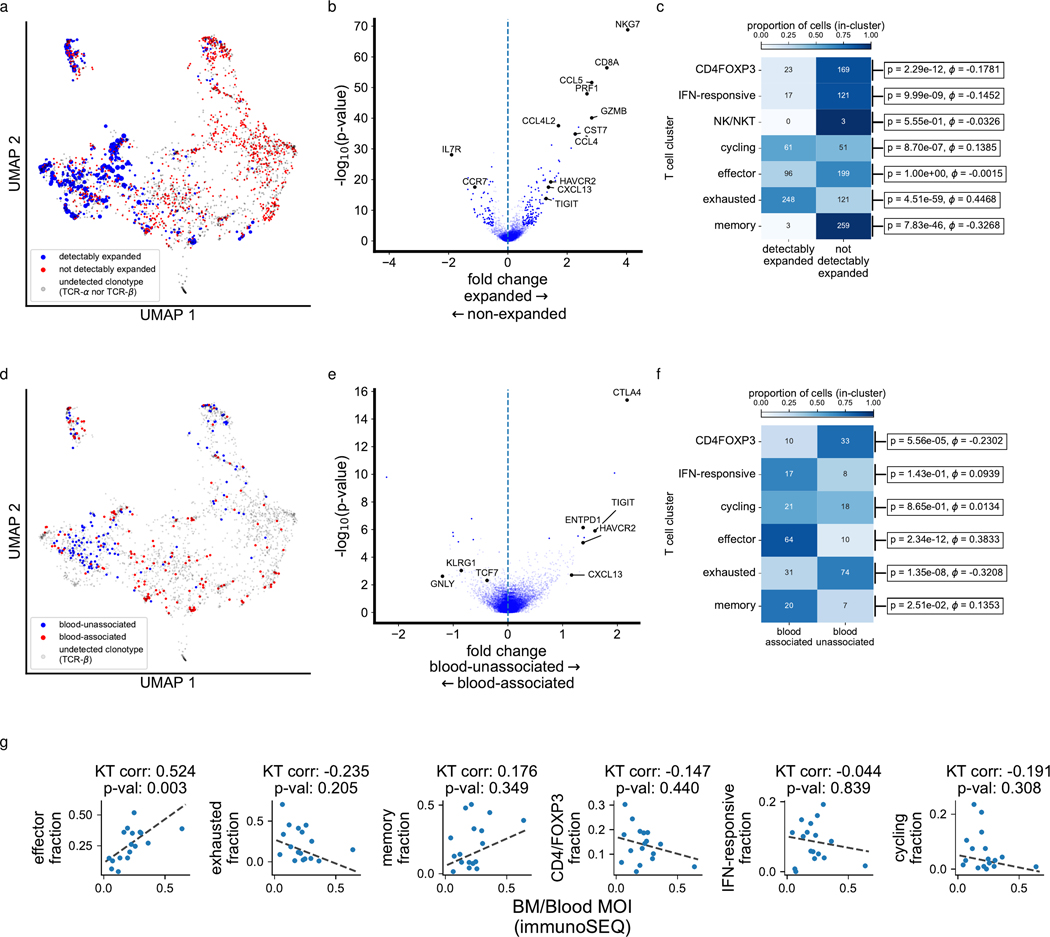
Melanoma-derived brain metastases (MBM) represent an unmet clinical need because central nervous system progression is frequently an end stage of the disease. Immune checkpoint inhibitors (ICI) provide a clinical opportunity against MBM; however, the MBM tumor microenvironment (TME) has not been fully elucidated in the context of ICI. To dissect unique elements of the MBM TME and correlates of MBM response to ICI, we collected 32 fresh MBM and performed single-cell RNA sequencing of the MBM TME and T-cell receptor clonotyping on T cells from MBM and matched blood and extracranial lesions. We observed myeloid phenotypic heterogeneity in the MBM TME, most notably multiple distinct neutrophil states, including an IL8-expressing population that correlated with malignant cell epithelial-to-mesenchymal transition. In addition, we observed significant relationships between intracranial T-cell phenotypes and the distribution of T-cell clonotypes intracranially and peripherally. We found that the phenotype, clonotype, and overall number of MBM-infiltrating T cells were associated with response to ICI, suggesting that ICI-responsive MBMs interact with peripheral blood in a manner similar to extracranial lesions. These data identify unique features of the MBM TME that may represent potential targets to improve clinical outcomes for patients with MBM.
©2022 American Association for Cancer Research.
Conflict of interest statement
Competing Interests
The other authors have no competing interests.
Figures

References
-
- Brastianos PK, Carter SL, Santagata S, Cahill DP, Taylor-Weiner A, Jones RT, et al. Genomic Characterization of Brain Metastases Reveals Branched Evolution and Potential Therapeutic Targets. Cancer Discov [Internet]. 2015 [cited 2018 Nov 11]; Available from: http://cancerdiscovery.aacrjournals.org/content/early/2015/10/14/2159-82... - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
