

Cognitive impairment is associated with greater preoperative symptoms, worse health-related quality of life, and reduced likelihood of recovery after cervical and lumbar spine surgery
- PMID: 35706693
- PMCID: PMC9189192
- DOI: 10.1016/j.xnsj.2022.100128
Cognitive impairment is associated with greater preoperative symptoms, worse health-related quality of life, and reduced likelihood of recovery after cervical and lumbar spine surgery
Abstract
Background: Cognitive impairment (CI) is associated with prolonged hospital stays and increased complications; however, its role in symptom severity and health-related quality of life (HRQoL) among spine patients is unknown. We determined 1) prevalence of preoperative CI; 2) associations between CI and preoperative pain, disability, and HRQoL; and 3) association between CI and postoperative improvements in HRQoL.
Methods: This is a prospective cohort study of 453 consecutive adult spine surgery patients between October 2019 and March 2021. We compared pain (Numeric Rating Scale, NRS), pain-related disability (Oswestry/Neck Disability Index, O/NDI), and HRQoL (PROMIS-29 profile, version 2.0) among participants having severe (PROMIS-29 Cognitive Abilities score ≤30), moderate (31-35), or mild CI (36-40) or who were unimpaired (score >40), using analysis of variance. Likelihood of clinical improvement given the presence of any CI was estimated using logistic regression. All comparisons were adjusted for age, gender, comorbidity, and use of opioid medication during the last 30 days. Alpha=.05.
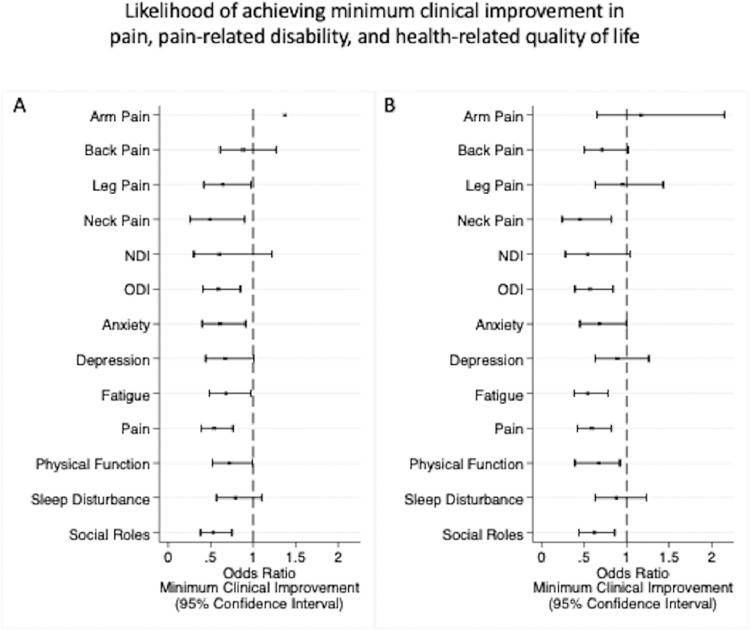
Results: Eighty-five respondents endorsed CI (38 mild; 27 moderate; 20 severe). Preoperatively, those with CI had more severe back pain (p=.005) and neck pain (p=.025) but no differences in leg or arm pain. Those with CI had greater disability on ODI (p<.001) and NDI (p<.001) and worse HRQoL in all domains (all, p<.001). At 6 and 12 months postoperatively, those with CI were less likely to experience clinical improvement in disability and HRQoL (anxiety, pain interference, physical function, and satisfaction with ability to participant in social roles) (all, p<.05).
Conclusions: CI was present in nearly 20% of spine patients before surgery and was independently associated with worse preoperative back and neck pain, disability, and HRQoL. Those with CI had approximately one-half the likelihood of achieving meaningful clinical improvement postoperatively. These results indicate a need to evaluate spine patients' cognitive impairment prior to surgery.
Level of evidence: III.
Keywords: Neck Disability Index; Oswestry Disability Index; Patient-Reported Outcome Measurement Information System; cognitive impairment; pain intensity Numeric Rating Scale; patient-reported outcomes; spine surgery.
© 2022 The Authors. Published by Elsevier Ltd on behalf of North American Spine Society.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

Similar articles
-
Persistent sleep disturbance after spine surgery is associated with failure to achieve meaningful improvements in pain and health-related quality of life.Spine J. 2021 Aug;21(8):1325-1331. doi: 10.1016/j.spinee.2021.03.021. Epub 2021 Mar 25. Spine J. 2021. PMID: 33774209
-
Recovery kinetics following spinal deformity correction: a comparison of isolated cervical, thoracolumbar, and combined deformity morphometries.Spine J. 2019 Aug;19(8):1422-1433. doi: 10.1016/j.spinee.2019.03.006. Epub 2019 Mar 28. Spine J. 2019. PMID: 30930292
-
Accurately measuring the quality and effectiveness of cervical spine surgery in registry efforts: determining the most valid and responsive instruments.Spine J. 2015 Jun 1;15(6):1203-9. doi: 10.1016/j.spinee.2013.07.444. Epub 2013 Sep 26. Spine J. 2015. PMID: 24076442
-
Despite worse baseline status depressed patients achieved outcomes similar to those in nondepressed patients after surgery for cervical deformity.Neurosurg Focus. 2017 Dec;43(6):E10. doi: 10.3171/2017.8.FOCUS17486. Neurosurg Focus. 2017. PMID: 29191101
-
Influence of Preoperative Depression on Cervical Spine Surgery Outcomes: A Systematic Review and Meta-Analysis.Global Spine J. 2025 Jun;15(5):2767-2778. doi: 10.1177/21925682251316245. Epub 2025 Jan 24. Global Spine J. 2025. PMID: 39853315 Free PMC article. Review.
Cited by
-
The Impact of COVID-19 Infection on Cognitive Function and the Implication for Rehabilitation: A Systematic Review and Meta-Analysis.Int J Environ Res Public Health. 2022 Jun 24;19(13):7748. doi: 10.3390/ijerph19137748. Int J Environ Res Public Health. 2022. PMID: 35805406 Free PMC article.
References
-
- Ali ZS, Ma TS, Ozturk AK, Malhotra NR, Schuster JM, Marcotte PJ, et al. Pre-optimization of spinal surgery patients: Development of a neurosurgical enhanced recovery after surgery (ERAS) protocol. Clinical Neurology and Neurosurgery. 2018;164:142–153. doi: 10.1016/j.clineuro.2017.12.003. - DOI - PubMed
-
- Adogwa O, Elsamadicy AA, Lydon E, Vuong VD, Cheng J, Karikari IO, et al. The prevalence of undiagnosed pre-surgical cognitive impairment and its post-surgical clinical impact in elderly patients undergoing surgery for adult spinal deformity. J Spine Surg. 2017;3:358–363. doi: 10.21037/jss.2017.07.01. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
