

The outcome of bioabsorbable staple line reinforcement versus standard stapler for distal pancreatectomy: A systematic review and meta-analysis
- PMID: 35708377
- PMCID: PMC9306122
- DOI: 10.4103/jmas.jmas_47_22
The outcome of bioabsorbable staple line reinforcement versus standard stapler for distal pancreatectomy: A systematic review and meta-analysis
Abstract
Background and aim: In the era of minimally invasive procedures and as a way to decrease the incidence of post-operative pancreatic fistula (POPF), the use of staplers for distal pancreatectomy (DP) has increased dramatically. Our aim was to investigate whether reinforced staplers decrease the incidence of clinically relevant PF after DP compared with staplers without reinforcement.
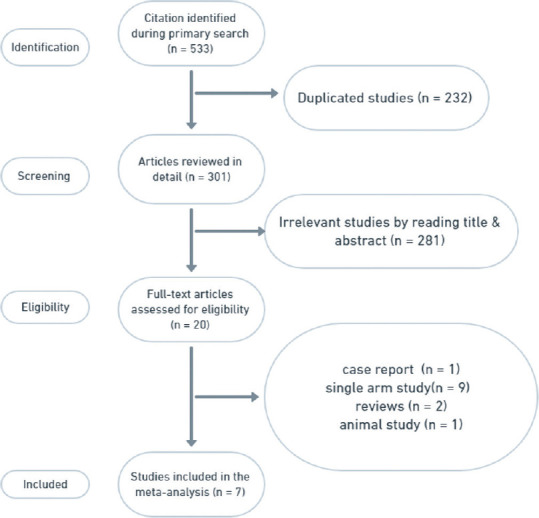
Methods: PubMed, Scopus, Web of Science and Cochrane Library were searched for eligible studies from inception to 1 November 2021, and a systematic review and a meta-analysis were done to detect the outcomes after using reinforced staplers versus standard stapler for DP.
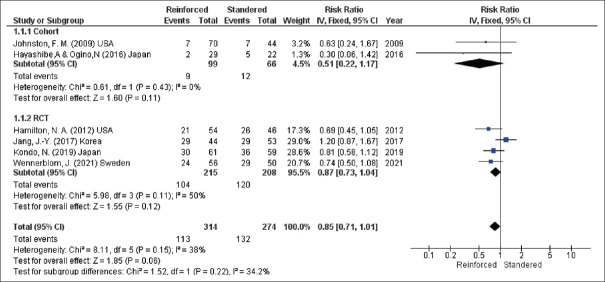
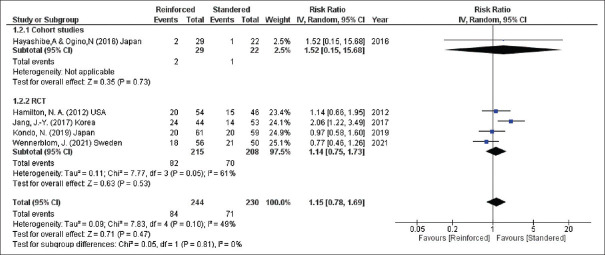
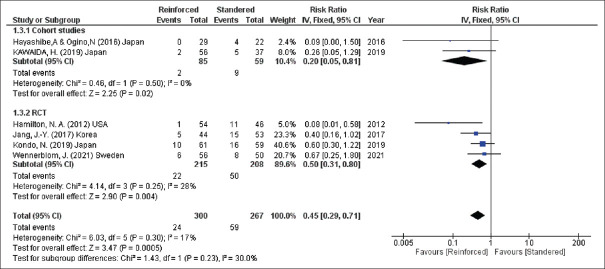
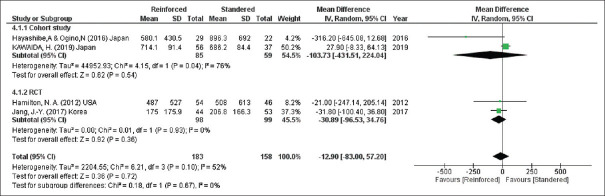
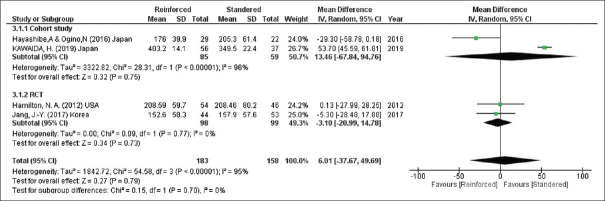
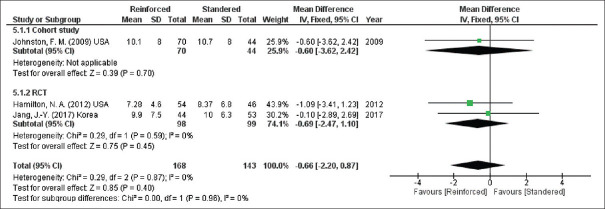
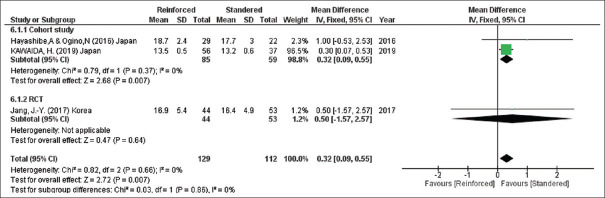
Results: Seven studies with a total of 681 patients were included. The overall incidence of POPF and the incidence of Grade A POPF after DP are similar for the two groups (overall POPF, risk ratio [RR] = 0.85, 95% confidence interval [CI] = 0.71-1.01, P = 0.06; I2 = 38% and Grade A POPF, RR = 1.15, 95% CI = 0.78-1.69, P = 0.47; I2 = 49%). However, the incidence of clinically significant POPF (Grades B and C) is significantly lower in DP with reinforced staplers than DP with bare staplers (Grades B and C, RR = 0.45, 95% CI = 0.29-0.71, P = 0.0005; I2 = 17%). Nevertheless, the time of the operation, the blood loss during surgical procedure, the hospital stay after the surgery and the thickness of the pancreas are similar for both techniques.
Conclusion: Although staple line reinforcement after DP failed to prevent biochemical PF, it significantly reduced the rate of clinically relevant POPF in comparison to standard stapling.
Keywords: Distal pancreatectomy; pancreatic fistula; reinforcement; stapler.
Conflict of interest statement
None
Figures
Similar articles
-
Efficacy of Reinforced Stapler for Preventing Postoperative Pancreatic Fistula After Minimally Invasive Distal Pancreatectomy.Anticancer Res. 2024 Aug;44(8):3655-3661. doi: 10.21873/anticanres.17189. Anticancer Res. 2024. PMID: 39060077
-
A Multicenter, Randomized, Controlled Trial Comparing Reinforced Staplers with Bare Staplers During Distal Pancreatectomy (HiSCO-07 Trial).Ann Surg Oncol. 2019 May;26(5):1519-1527. doi: 10.1245/s10434-019-07222-0. Epub 2019 Feb 19. Ann Surg Oncol. 2019. PMID: 30783854 Clinical Trial.
-
Reinforced staplers for distal pancreatectomy.Langenbecks Arch Surg. 2017 Dec;402(8):1197-1204. doi: 10.1007/s00423-017-1634-1. Epub 2017 Nov 4. Langenbecks Arch Surg. 2017. PMID: 29103084 Clinical Trial.
-
Meta-analysis and trial sequential analysis of pancreatic stump closure using a hand-sewn or stapler technique in distal pancreatectomy.Ann Hepatobiliary Pancreat Surg. 2024 Aug 31;28(3):302-314. doi: 10.14701/ahbps.24-015. Epub 2024 Mar 25. Ann Hepatobiliary Pancreat Surg. 2024. PMID: 38522846 Free PMC article. Review.
-
Attempts to prevent postoperative pancreatic fistula after distal pancreatectomy.Surg Today. 2017 Apr;47(4):416-424. doi: 10.1007/s00595-016-1367-8. Epub 2016 Jun 20. Surg Today. 2017. PMID: 27324393 Review.
Cited by
-
The efficacy of wrapping with polyglycolic acid mesh and fibrin glue in preventing clinically relevant pancreatic fistula after minimally invasive distal pancreatectomy (WRAP Study): study protocol for a multicenter randomized controlled trial in Japan.BMC Surg. 2024 Oct 16;24(1):314. doi: 10.1186/s12893-024-02610-0. BMC Surg. 2024. PMID: 39415231 Free PMC article.
-
Reinforced stapling does not reduce postoperative pancreatic fistula in distal pancreatectomy: a systematic review and meta-analysis.Updates Surg. 2023 Dec;75(8):2063-2074. doi: 10.1007/s13304-023-01691-5. Epub 2023 Nov 10. Updates Surg. 2023. PMID: 37950142
-
The clinical effectiveness of staple line reinforcement with different matrix used in surgery.Front Bioeng Biotechnol. 2023 Jun 7;11:1178619. doi: 10.3389/fbioe.2023.1178619. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 37351469 Free PMC article. Review.
-
Intraoperative Video Analysis of Pancreatic Stump and Stapler Closure-Induced Pancreatic Fistula in Laparoscopic Distal Pancreatectomy: A Retrospective Study.Cureus. 2024 Apr 24;16(4):e58959. doi: 10.7759/cureus.58959. eCollection 2024 Apr. Cureus. 2024. PMID: 38800290 Free PMC article.
References
-
- Adam U, Makowiec F, Riediger H, Benz S, Liebe S, Hopt UT. Pancreatic leakage after pancreas resection. An analysis of 345 operated patients. Chirurg. 2002;73:466–73. - PubMed
-
- Sarr MG, Group TP. The potent somatostatin analogue vapreotide does not decrease pancreas-specific complications after elective pancreatectomy: A prospective, multicenter, double-blinded, randomized, placebo-controlled trial. J Am Coll Surg. 2003;196:556–64. - PubMed
-
- Frozanpor F, Lundell L, Segersvärd R, Arnelo U. The effect of prophylactic transpapillary pancreatic stent insertion on clinically significant leak rate following distal pancreatectomy: Results of a prospective controlled clinical trial. Ann Surg. 2012;255:1032–6. - PubMed
-
- Hassenpflug M, Hinz U, Strobel O, Volpert J, Knebel P, Diener MK, et al. Teres ligament patch reduces relevant morbidity after distal pancreatectomy (the DISCOVER Randomized Controlled Trial) Ann Surg. 2016;264:723–30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
