

Changes in Optic Nerve Head and Retinal Morphology During Spaceflight and Acute Fluid Shift Reversal
- PMID: 35708665
- PMCID: PMC9204621
- DOI: 10.1001/jamaophthalmol.2022.1946
Changes in Optic Nerve Head and Retinal Morphology During Spaceflight and Acute Fluid Shift Reversal
Erratum in
-
Correction to Data Points in Figure.JAMA Ophthalmol. 2022 Sep 1;140(9):912. doi: 10.1001/jamaophthalmol.2022.3302. JAMA Ophthalmol. 2022. PMID: 35951337 Free PMC article. No abstract available.
Abstract
Importance: Countermeasures that reverse the headward fluid shift experienced in weightlessness have the potential to mitigate spaceflight-associated neuro-ocular syndrome. This study investigated whether use of the countermeasure lower-body negative pressure during spaceflight was associated with changes in ocular structure.
Objective: To determine whether changes to the optic nerve head and retina during spaceflight can be mitigated by brief in-flight application of 25-mm Hg lower-body negative pressure.
Design, setting, and participants: In the National Aeronautics and Space Administration's "Fluid Shifts Study," a prospective cohort study, optical coherence tomography scans of the optic nerve head and macula were obtained from US and international crew members before flight, in-flight, and up to 180 days after return to Earth. In-flight scans were obtained both under normal weightless conditions and 10 to 20 minutes into lower-body negative pressure exposure. Preflight and postflight data were collected in the seated, supine, and head-down tilt postures. Crew members completed 6- to 12-month missions that took place on the International Space Station. Data were analyzed from 2016 to 2021.
Interventions or exposures: Spaceflight and lower-body negative pressure.
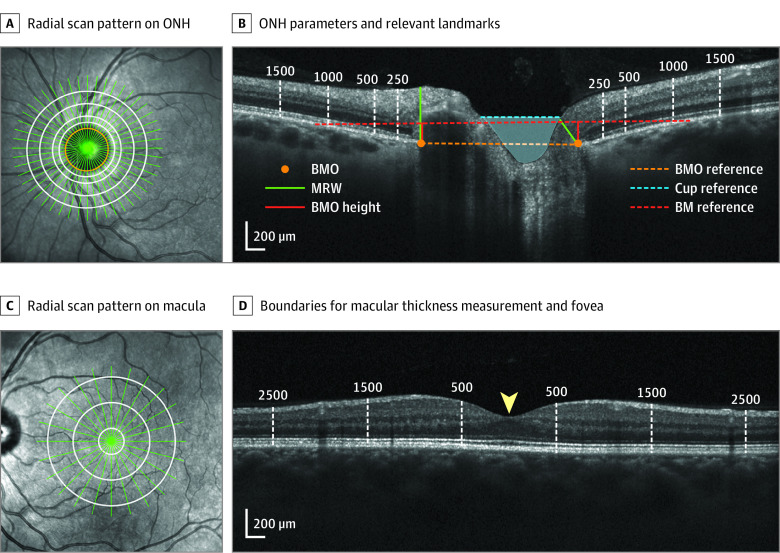
Main outcomes and measures: Changes in minimum rim width, optic cup volume, Bruch membrane opening height, peripapillary total retinal thickness, and macular thickness.
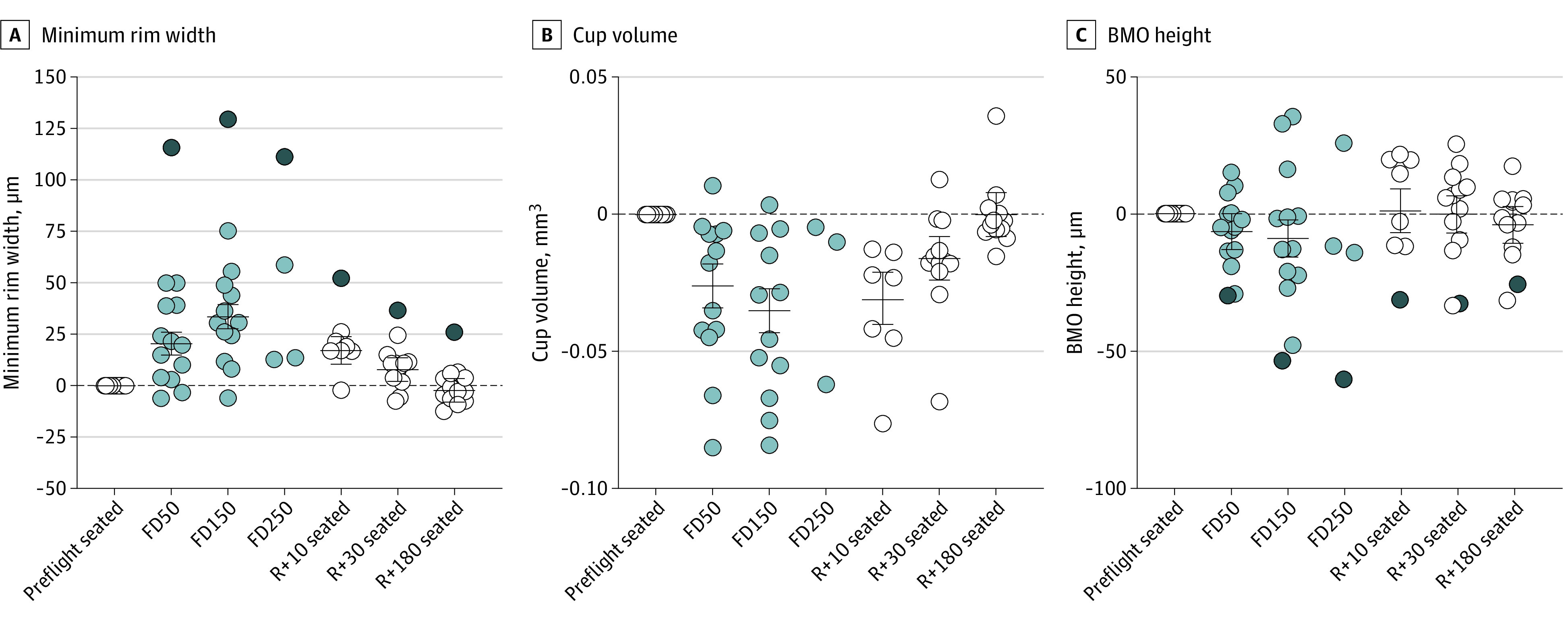
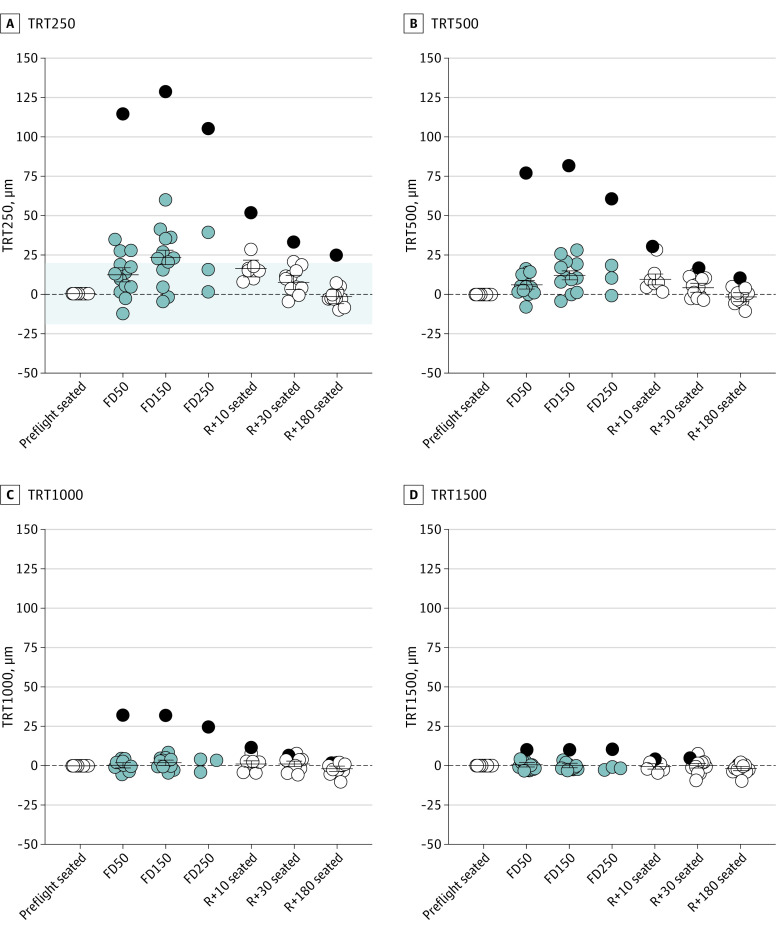
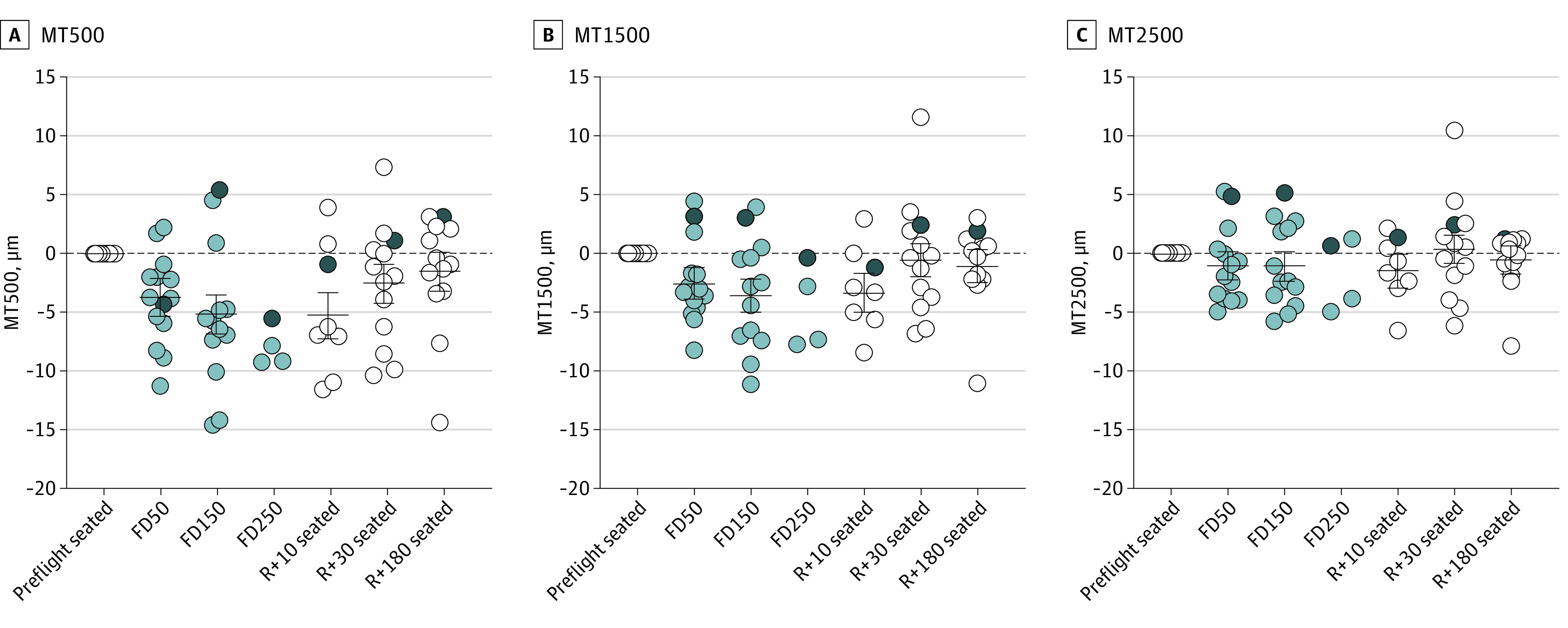
Results: Mean (SD) flight duration for the 14 crew members (mean [SD] age, 45 [6] years; 11 male crew members [79%]) was 214 (72) days. Ocular changes on flight day 150, as compared with preflight seated, included an increase in minimum rim width (33.8 μm; 95% CI, 27.9-39.7 μm; P < .001), decrease in cup volume (0.038 mm3; 95% CI, 0.030-0.046 mm3; P < .001), posterior displacement of Bruch membrane opening (-9.0 μm; 95% CI, -15.7 to -2.2 μm; P = .009), and decrease in macular thickness (fovea to 500 μm, 5.1 μm; 95% CI, 3.5-6.8 μm; P < .001). Brief exposure to lower-body negative pressure did not affect these parameters.
Conclusions and relevance: Results of this cohort study suggest that peripapillary tissue thickening, decreased cup volume, and mild central macular thinning were associated with long-duration spaceflight. Acute exposure to 25-mm Hg lower-body negative pressure did not alter optic nerve head or retinal morphology, suggesting that longer durations of a fluid shift reversal may be needed to mitigate spaceflight-induced changes and/or other factors are involved.
Conflict of interest statement
Figures
Comment in
-
The Enigma of the Posterior Displacement of the Bruch Membrane Opening During Spaceflight-Reply.JAMA Ophthalmol. 2022 Oct 1;140(10):1029-1030. doi: 10.1001/jamaophthalmol.2022.3634. JAMA Ophthalmol. 2022. PMID: 36107438 No abstract available.
-
The Enigma of the Posterior Displacement of the Bruch Membrane Opening During Spaceflight.JAMA Ophthalmol. 2022 Oct 1;140(10):1029. doi: 10.1001/jamaophthalmol.2022.3637. JAMA Ophthalmol. 2022. PMID: 36107439 No abstract available.
