

Association of High Tumor Mutation Burden in Non-Small Cell Lung Cancers With Increased Immune Infiltration and Improved Clinical Outcomes of PD-L1 Blockade Across PD-L1 Expression Levels
- PMID: 35708671
- PMCID: PMC9204620
- DOI: 10.1001/jamaoncol.2022.1981
Association of High Tumor Mutation Burden in Non-Small Cell Lung Cancers With Increased Immune Infiltration and Improved Clinical Outcomes of PD-L1 Blockade Across PD-L1 Expression Levels
Erratum in
-
Error in Figure Axis Label.JAMA Oncol. 2022 Nov 1;8(11):1702. doi: 10.1001/jamaoncol.2022.5957. JAMA Oncol. 2022. PMID: 36394573 Free PMC article. No abstract available.
Abstract
Importance: Although tumor mutation burden (TMB) has been explored as a potential biomarker of immunotherapy efficacy in solid tumors, there still is a lack of consensus about the optimal TMB threshold that best discriminates improved outcomes of immune checkpoint inhibitor therapy among patients with non-small cell lung cancer (NSCLC).
Objectives: To determine the association between increasing TMB levels and immunotherapy efficacy across clinically relevant programmed death ligand-1 (PD-L1) levels in patients with NSCLC.
Design, setting, and participants: This multicenter cohort study included patients with advanced NSCLC treated with immunotherapy who received programmed cell death-1 (PD-1) or PD-L1 inhibition in the Dana-Farber Cancer Institute (DFCI), Memorial Sloan Kettering Cancer Center (MSKCC), and in the Stand Up To Cancer (SU2C)/Mark Foundation data sets. Clinicopathological and genomic data were collected from patients between September 2013 and September 2020. Data analysis was performed from November 2021 to February 2022.
Exposures: Treatment with PD-1/PD-L1 inhibition without chemotherapy.
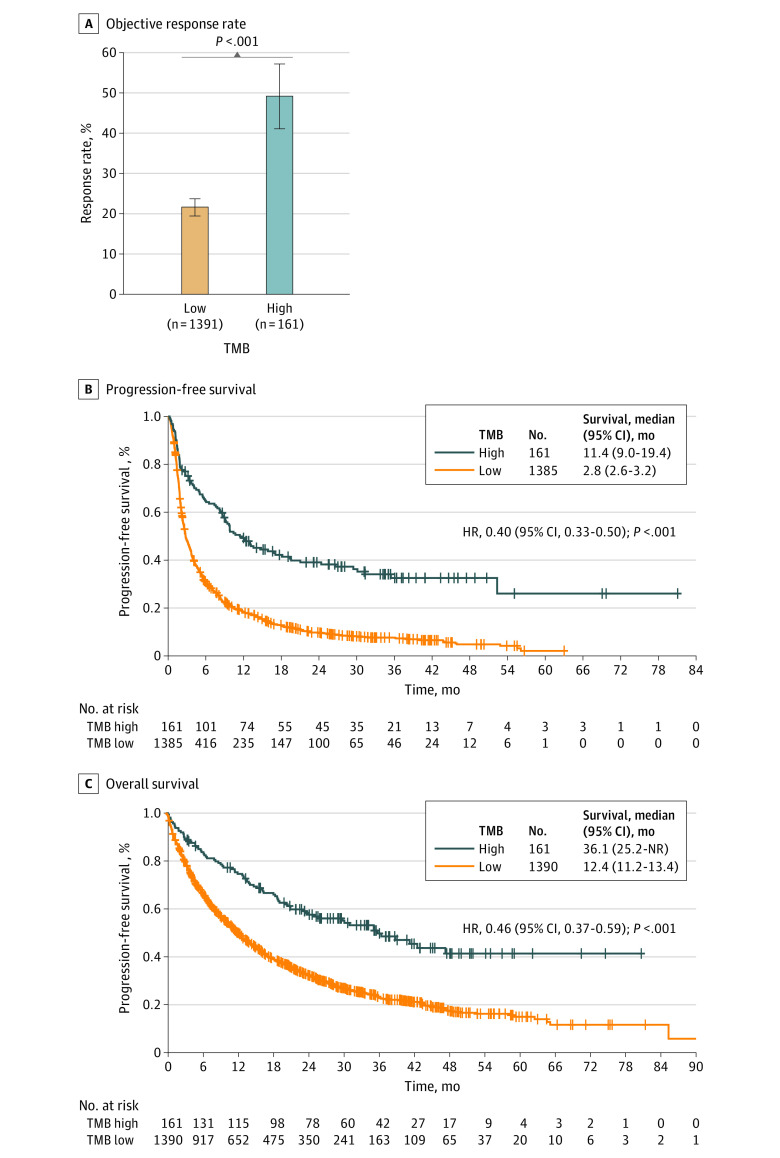
Main outcomes and measures: Association of TMB levels with objective response rate (ORR), progression-free survival (PFS), and overall survival (OS).
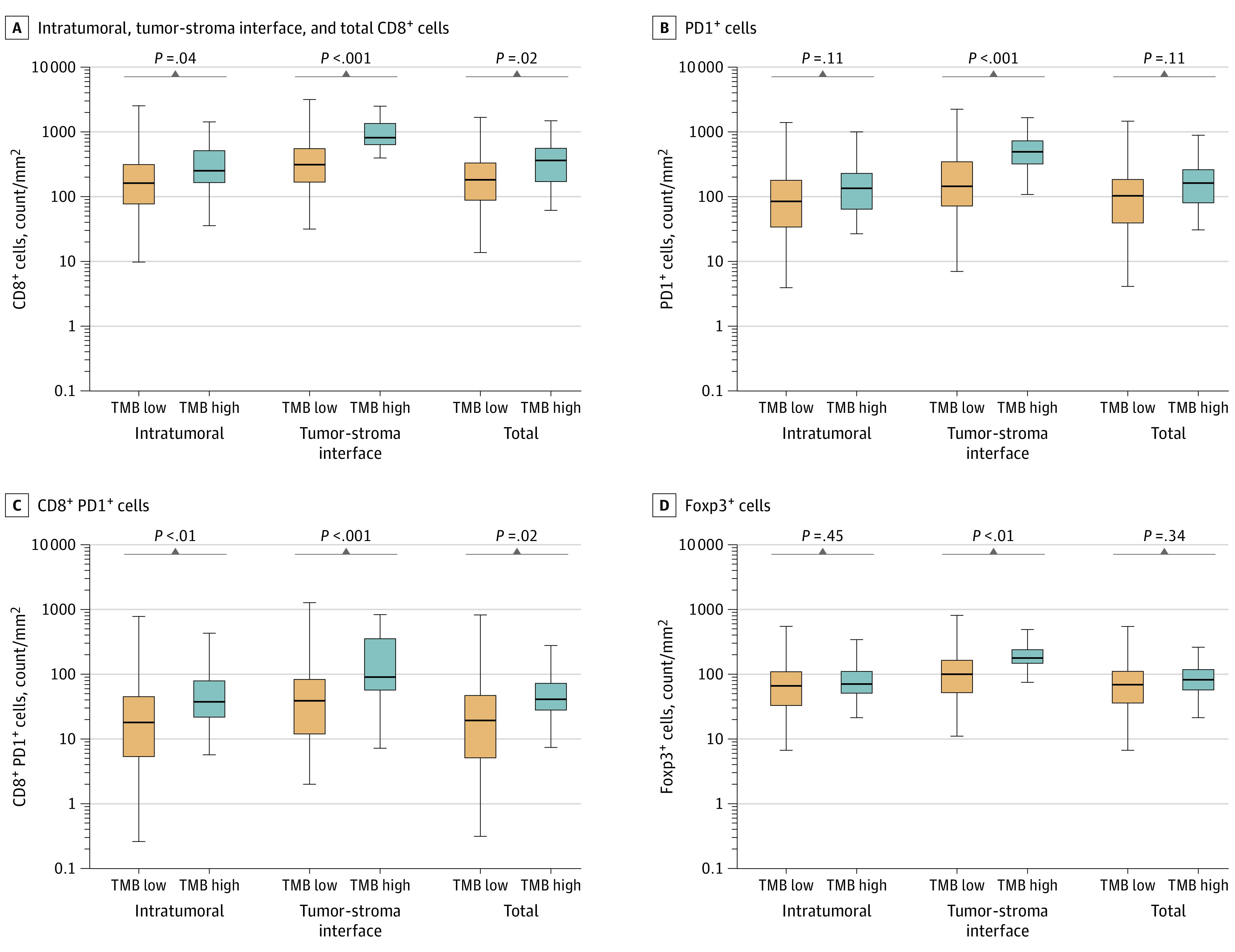
Results: In the entire cohort of 1552 patients with advanced NSCLC who received PD-1/PD-L1 blockade, the median (range) age was 66 (22-92) years, 830 (53.5%) were women, and 1347 (86.8%) had cancer with nonsquamous histologic profile. A regression tree modeling ORR as a function of TMB identified 2 TMB groupings in the discovery cohort (MSKCC), defined as low TMB (≤19.0 mutations per megabase) and high TMB (>19.0 mutations per megabase), which were associated with increasing improvements in ORR, PFS, and OS in the discovery cohort and in 2 independent cohorts (DFCI and SU2C/Mark Foundation). These TMB levels also were associated with significant improvements in outcomes of immunotherapy in each PD-L1 tumor proportion score subgroup of less than 1%, 1% to 49%, and 50% or higher. The ORR to PD-1/PD-L1 inhibition was as high as 57% in patients with high TMB and PD-L1 expression 50% or higher and as low as 8.7% in patients with low TMB and PD-L1 expression less than 1%. Multiplexed immunofluorescence and transcriptomic profiling revealed that high TMB levels were associated with increased CD8-positive, PD-L1-positive T-cell infiltration, increased PD-L1 expression on tumor and immune cells, and upregulation of innate and adaptive immune response signatures.
Conclusions and relevance: These findings suggest that increasing TMB levels are associated with immune cell infiltration and an inflammatory T-cell-mediated response, resulting in increased sensitivity to PD-1/PD-L1 blockade in NSCLC across PD-L1 expression subgroups.
Conflict of interest statement
Figures
Comment in
-
Increased Tumor Mutation Burden Levels and Sensitivity of Non-Small Cell Lung Cancer to PD-L1 Blockade.JAMA Oncol. 2023 Apr 1;9(4):569-570. doi: 10.1001/jamaoncol.2022.7583. JAMA Oncol. 2023. PMID: 36729440 No abstract available.
-
Increased Tumor Mutation Burden Levels and Sensitivity of Non-Small Cell Lung Cancer to PD-L1 Blockade.JAMA Oncol. 2023 Apr 1;9(4):570. doi: 10.1001/jamaoncol.2022.7586. JAMA Oncol. 2023. PMID: 36729466 No abstract available.
References
-
- Mok TSK, Wu YL, Kudaba I, et al. ; KEYNOTE-042 Investigators . Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819-1830. doi: 10.1016/S0140-6736(18)32409-7 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
