

Two years later: Is the SARS-CoV-2 pandemic still having an impact on emergency surgery? An international cross-sectional survey among WSES members
- PMID: 35710386
- PMCID: PMC9202986
- DOI: 10.1186/s13017-022-00424-0
Two years later: Is the SARS-CoV-2 pandemic still having an impact on emergency surgery? An international cross-sectional survey among WSES members
Erratum in
-
Correction to: Two years later: Is the SARS-CoV-2 pandemic still having an impact on emergency surgery? An international cross-sectional survey among WSES members.World J Emerg Surg. 2022 Jul 8;17(1):39. doi: 10.1186/s13017-022-00442-y. World J Emerg Surg. 2022. PMID: 35804425 Free PMC article. No abstract available.
Abstract
Background: The SARS-CoV-2 pandemic is still ongoing and a major challenge for health care services worldwide. In the first WSES COVID-19 emergency surgery survey, a strong negative impact on emergency surgery (ES) had been described already early in the pandemic situation. However, the knowledge is limited about current effects of the pandemic on patient flow through emergency rooms, daily routine and decision making in ES as well as their changes over time during the last two pandemic years. This second WSES COVID-19 emergency surgery survey investigates the impact of the SARS-CoV-2 pandemic on ES during the course of the pandemic.
Methods: A web survey had been distributed to medical specialists in ES during a four-week period from January 2022, investigating the impact of the pandemic on patients and septic diseases both requiring ES, structural problems due to the pandemic and time-to-intervention in ES routine.
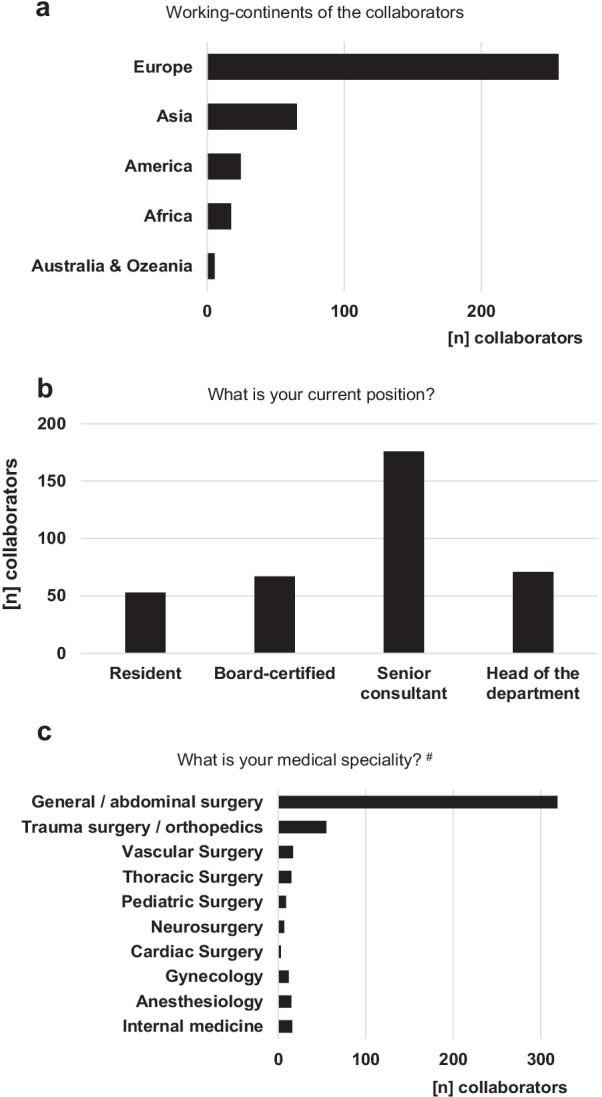
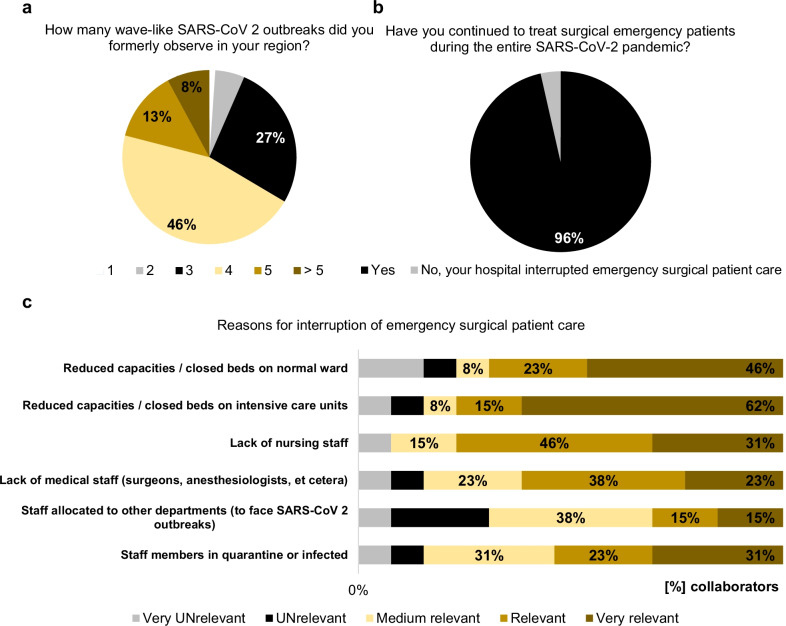
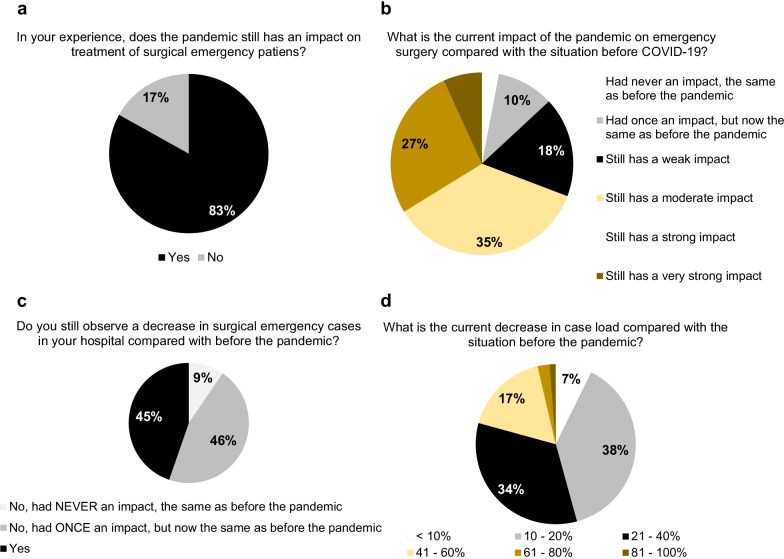
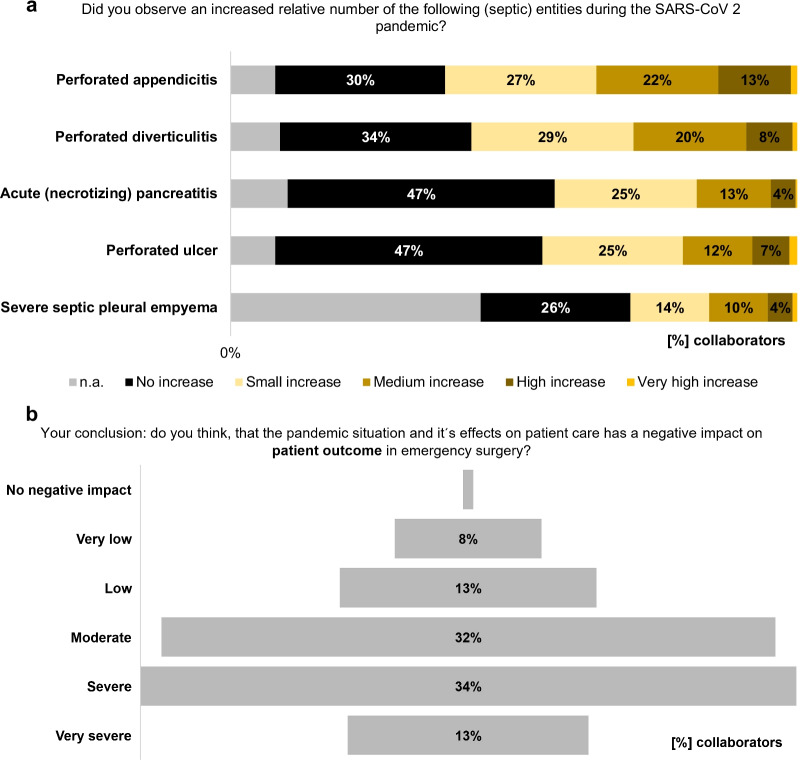
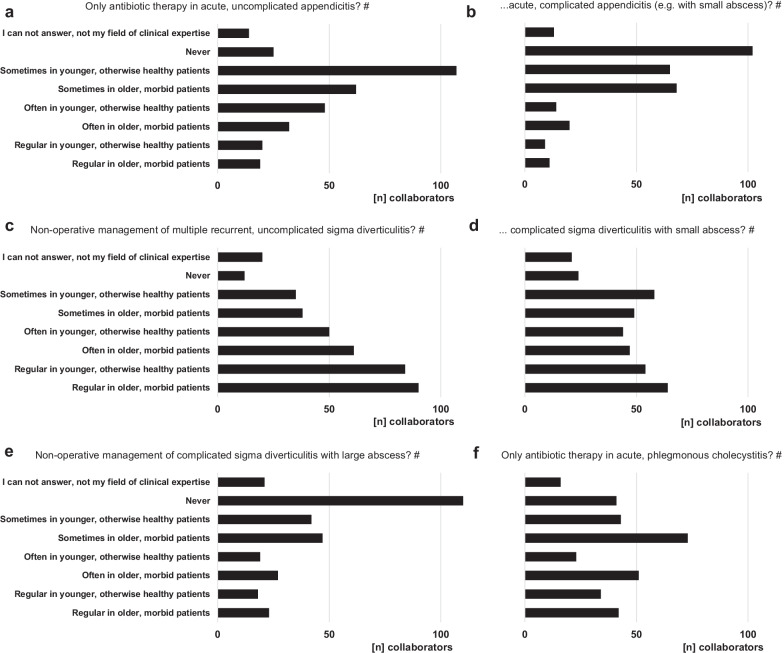
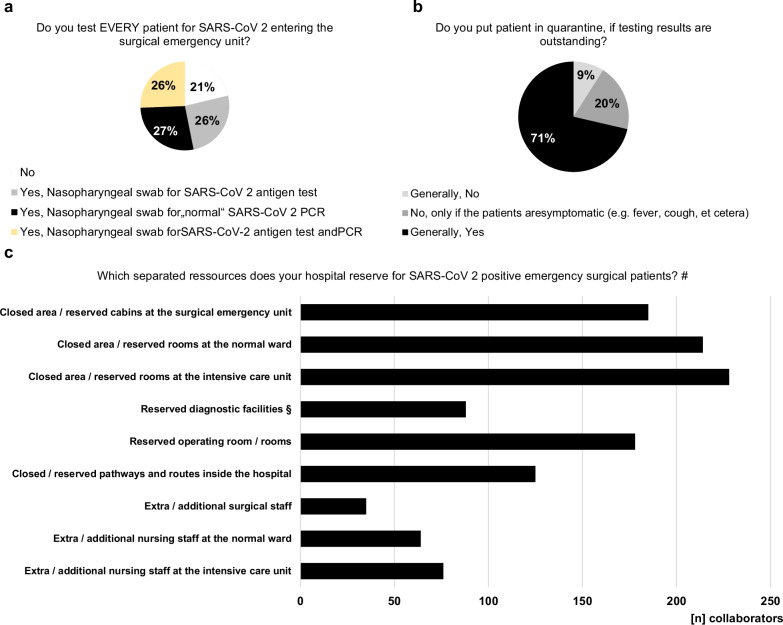
Results: 367 collaborators from 59 countries responded to the survey. The majority indicated that the pandemic still significantly impacts on treatment and outcome of surgical emergency patients (83.1% and 78.5%, respectively). As reasons, the collaborators reported decreased case load in ES (44.7%), but patients presenting with more prolonged and severe diseases, especially concerning perforated appendicitis (62.1%) and diverticulitis (57.5%). Otherwise, approximately 50% of the participants still observe a delay in time-to-intervention in ES compared with the situation before the pandemic. Relevant causes leading to enlarged time-to-intervention in ES during the pandemic are persistent problems with in-hospital logistics, lacks in medical staff as well as operating room and intensive care capacities during the pandemic. This leads not only to the need for triage or transferring of ES patients to other hospitals, reported by 64.0% and 48.8% of the collaborators, respectively, but also to paradigm shifts in treatment modalities to non-operative approaches reported by 67.3% of the participants, especially in uncomplicated appendicitis, cholecystitis and multiple-recurrent diverticulitis.
Conclusions: The SARS-CoV-2 pandemic still significantly impacts on care and outcome of patients in ES. Well-known problems with in-hospital logistics are not sufficiently resolved by now; however, medical staff shortages and reduced capacities have been dramatically aggravated over last two pandemic years.
Keywords: Appendicitis; COVID-19; Capacity; Emergency; Emergency surgery; Pandemic; Quarantine; SARS-CoV-2; Time to intervention; WSES.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
