

A registry of achondroplasia: a 6-year experience from the Czechia and Slovak Republic
- PMID: 35710503
- PMCID: PMC9205086
- DOI: 10.1186/s13023-022-02374-x
A registry of achondroplasia: a 6-year experience from the Czechia and Slovak Republic
Abstract
Background: Achondroplasia (ACH) is one of the most prevalent genetic forms of short-limbed skeletal dysplasia, caused by gain-of-function mutations in the receptor tyrosine kinase FGFR3. In August 2021, the C-type natriuretic peptide (CNP) analog vosoritide was approved for the treatment of ACH. A total of six other inhibitors of FGFR3 signaling are currently undergoing clinical evaluation for ACH. This progress creates an opportunity for children with ACH, who may gain early access to the treatment by entering clinical trials before the closure of their epiphyseal growth plates and cessation of growth. Pathophysiology associated with the ACH, however, demands a long observational period before admission to the interventional trial. Public patient registries can facilitate the process by identification of patients suitable for treatment and collecting the data necessary for the trial entry.
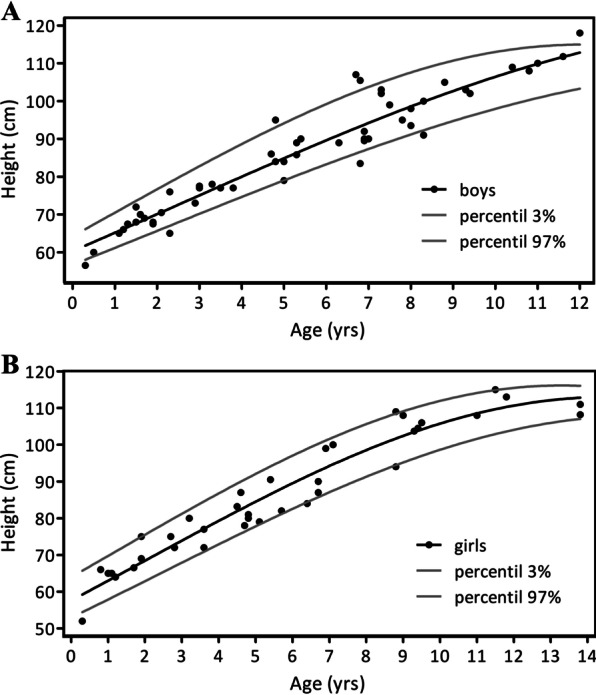
Results: In 2015, we established the prospective ACH registry in the Czechia and the Slovak Republic ( http://www.achondroplasia-registry.cz ). Patient data is collected through pediatric practitioners and other relevant specialists. After informed consent is given, the data is entered to the online TrialDB system and stored in the Oracle 9i database. The initial cohort included 51 ACH children (average age 8.5 years, range 3 months to 14 years). The frequency of selected neurological, orthopedic, or ORL diagnoses is also recorded. In 2015-2021, a total of 89 measurements of heights, weights, and other parameters were collected. The individual average growth rate was calculated and showed values without exception in the lower decile for the appropriate age. Evidence of paternal age effect was found, with 58.7% of ACH fathers older than the general average paternal age and 43.5% of fathers older by two or more years. One ACH patient had orthopedic limb extension and one patient received growth hormone therapy. Low blood pressure or renal impairment were not found in any patient.
Conclusion: The registry collected the clinical information of 51 pediatric ACH patients during its 6 years of existence, corresponding to ~ 60% of ACH patients living in the Czechia and Slovak Republic. The registry continues to collect ACH patient data with annual frequency to monitor the growth and other parameters in preparation for future therapy.
Keywords: Achondroplasia; FGFR3; ReACH; Registry; Skeletal dysplasia; Treatment.
© 2022. The Author(s).
Conflict of interest statement
The authors have no competing interests.
Figures

Similar articles
-
C-Type Natriuretic Peptide Analog as Therapy for Achondroplasia.Endocr Dev. 2016;30:98-105. doi: 10.1159/000439334. Epub 2015 Dec 10. Endocr Dev. 2016. PMID: 26684019 Review.
-
Maternal administration of meclozine for the treatment of foramen magnum stenosis in transgenic mice with achondroplasia.J Neurosurg Pediatr. 2017 Jan;19(1):91-95. doi: 10.3171/2016.7.PEDS16199. Epub 2016 Oct 21. J Neurosurg Pediatr. 2017. PMID: 27767902
-
Novel phenotype of achondroplasia due to biallelic FGFR3 pathogenic variants.Am J Med Genet A. 2018 Jul;176(7):1675-1679. doi: 10.1002/ajmg.a.38839. Am J Med Genet A. 2018. PMID: 30160829 Free PMC article.
-
Promising horizons in achondroplasia along with the development of new drugs.Endocr J. 2024 Jul 12;71(7):643-650. doi: 10.1507/endocrj.EJ24-0109. Epub 2024 Apr 4. Endocr J. 2024. PMID: 38569854 Review.
-
Knock-in human FGFR3 achondroplasia mutation as a mouse model for human skeletal dysplasia.Sci Rep. 2017 Feb 23;7:43220. doi: 10.1038/srep43220. Sci Rep. 2017. PMID: 28230213 Free PMC article.
Cited by
-
Integrating vosoritide therapy with limb surgery in paediatric patients with achondroplasia: real-life experiences.Orphanet J Rare Dis. 2025 Jul 17;20(1):369. doi: 10.1186/s13023-025-03853-7. Orphanet J Rare Dis. 2025. PMID: 40676599 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
