

Dual-Layer Rotation: A Versatile Therapeutic Mammoplasty Technique
- PMID: 35711016
- PMCID: PMC9492593
- DOI: 10.1245/s10434-022-11977-4
Dual-Layer Rotation: A Versatile Therapeutic Mammoplasty Technique
Abstract
Background: Multifocal or complex breast lesions are a challenge for breast-conserving surgery, particularly surgery in small breasts or those located in the upper inner quadrant. The dual-layer rotation technique exploits the idea of manipulating the skin and glandular tissue in separate layers to fill the resection cavity via vertical mammoplasty if skin excision is not required, except in the central area.
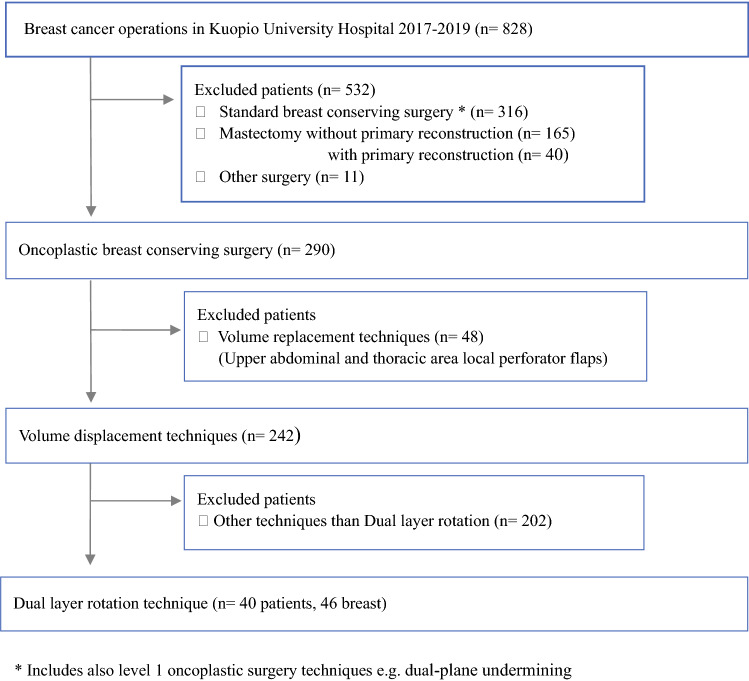
Methods: The authors performed a retrospective review of consecutive breast cancer patients who underwent DLR mammoplasty between 2017 and 2019 at a single institution. Clinical data, reoperations, surgical complications, delays in adjuvant treatments, and the need for late revisional surgery were evaluated. Aesthetic outcomes were evaluated objectively and subjectively from photographs.
Results: The study included 46 breasts of 40 patients. Tumors were located in the UIQ (30%, 14/46) or in multiple quadrants (22%, 10/46). One third (33%, 13/40) of the patients had a small breast cup size (A-B). Negative margins were primarily achieved in 45 of the 46 breasts. Major complications occurred in three patients, who needed reoperation, and adjuvant therapy was delayed for one of these patients. Late refinement surgery was needed for two patients. The objective and subjective aesthetic outcomes were good or excellent regardless of the tumor position.
Conclusion: As a novel oncoplastic approach, DLR mammoplasty offers a one-step procedure to treat selected breast cancer patients with challenging resection defects due to different breast sizes or lesion locations. The technique preserves the breast's natural appearance.
© 2022. The Author(s).
Conflict of interest statement
There are no conflicts of interest.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
