

Modified Interpretations of the Supine Roll Test in Horizontal Canal BPPV Based on Simulations: How the Initial Position of the Debris in the Canal and the Sequence of Testing Affects the Direction of the Nystagmus and the Diagnosis
- PMID: 35711266
- PMCID: PMC9197467
- DOI: 10.3389/fneur.2022.881156
Modified Interpretations of the Supine Roll Test in Horizontal Canal BPPV Based on Simulations: How the Initial Position of the Debris in the Canal and the Sequence of Testing Affects the Direction of the Nystagmus and the Diagnosis
Abstract
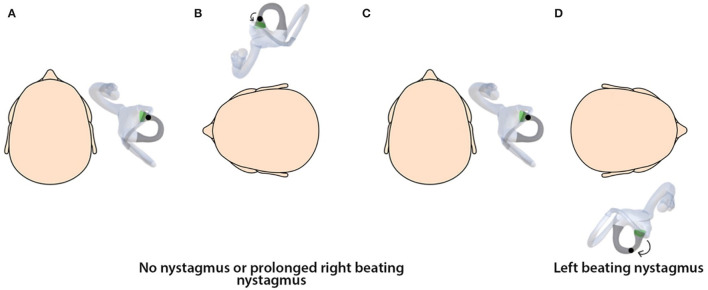
Background and objectives: The aim of this study was to show with three-dimensional simulations how the diagnostic supine roll test (SRT) is affected by the initial position of the debris within the horizontal canal (hc) and study the nystagmus patterns on changing the sequence of testing and its impact on the diagnosis of the side of involvement in hc-BPPV.
Methods: A 3D dynamic simulation model was developed and applied based on reconstructed MRI images and fluid dynamics. Each semicircular canal was linked to the respective extraocular muscles to visualize nystagmus generated on stimulation of the canal.
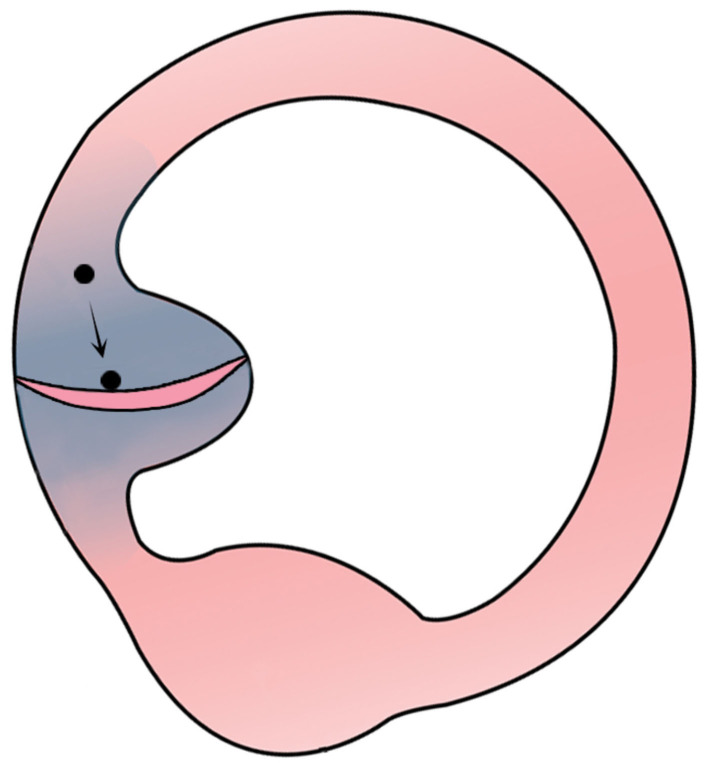
Results: The simulations of hc-canalithiasis showed that the nystagmus pattern seen with the SRT is changed by the initial position of the otolith debris within the canal and the sequence of testing. The debris changes position during SRT so that sequential steps do not start at the initial position as previously assumed. The sequence of performing the SRT steps from the right or left side influences the nystagmus pattern generated: bilateral direction-changing, bilateral direction-fixed, and unilateral nystagmus can be seen in different test conditions. The SRT itself may even reposition the debris out of the canal.
Conclusions and clinical implications: Simulations provide a dynamic tool to study the diagnostic SRT in hc-canalithiasis. Starting the SRT from right or left has a major impact on the test outcome (unlike the Dix-Hallpike maneuver). The findings provide a new interpretation for the results of the SRT. The simulations explain the phenomenon of direction-fixed nystagmus as a logical consequence of starting the SRT with the head turned toward the non-affected side in hc-canalithiasis with debris in the ampullary arm. They also show that unilateral nystagmus seen on SRT indicates canalithiasis of the non-ampullary arm of the side opposite to the side of nystagmus. The generation of bilateral direction-changing, bilateral direction-fixed, and unilateral nystagmus can be the cause of misdiagnoses in terms of the affected side and underlying mechanisms. Finally, a recommendation for a standardized protocol for the sequence of positional tests should be established to ensure uniform interpretation of test results.
Keywords: BPPV; canalithiasis; horizontal canal; maneuvers; nystagmus; simulation; supine roll test.
Copyright © 2022 Bhandari, Bhandari, Kingma and Strupp.
Conflict of interest statement
MS is the joint chief editor of the Journal of Neurology, editor in chief of Frontiers of Neuro-otology and section editor of F1000. He has received speaker's honoraria from Abbott, Auris Medical, Biogen, Eisai, Grünenthal, GSK, Henning Pharma, Interacoustics, J&J, MSD, Otometrics, Pierre-Fabre, TEVA, UCB, and Viatris. He is a shareholder and investor of IntraBio. He distributes “M-glasses” and “Positional vertigo App.” He acts as a consultant for Abbott, AurisMedical, Heel, IntraBio, and Sensorion. RB is the director of NeuroEquilibrium Diagnostic Systems Private Limited, India. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources