

Continuous Endogenous Exhaled CO Monitoring by Laser Spectrometer in Human EVLP Before Lung Transplantation
- PMID: 35711322
- PMCID: PMC9192958
- DOI: 10.3389/ti.2022.10455
Continuous Endogenous Exhaled CO Monitoring by Laser Spectrometer in Human EVLP Before Lung Transplantation
Abstract
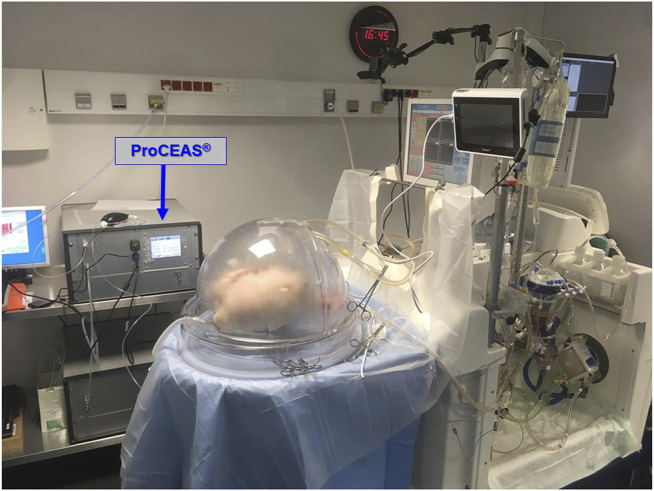
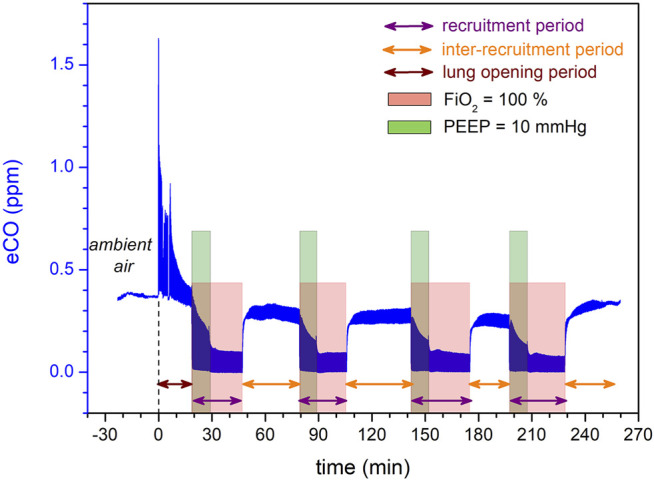
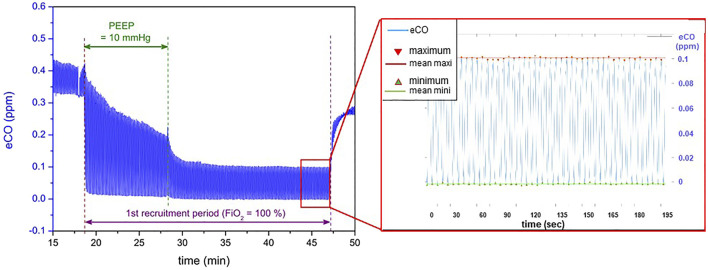
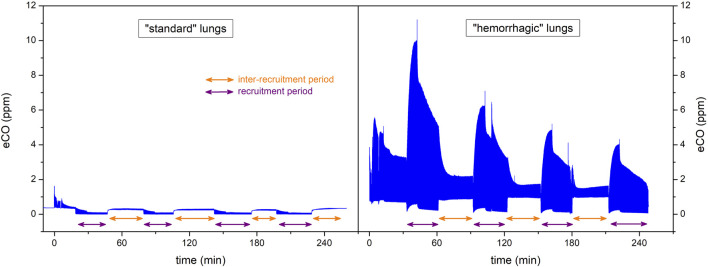
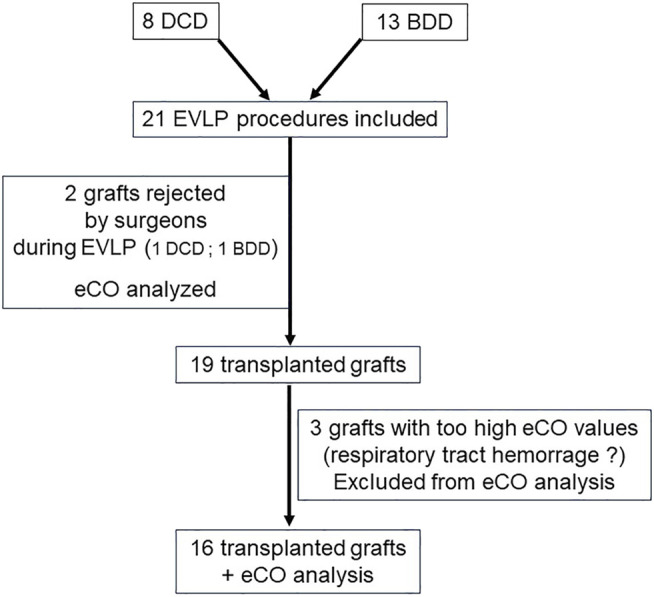
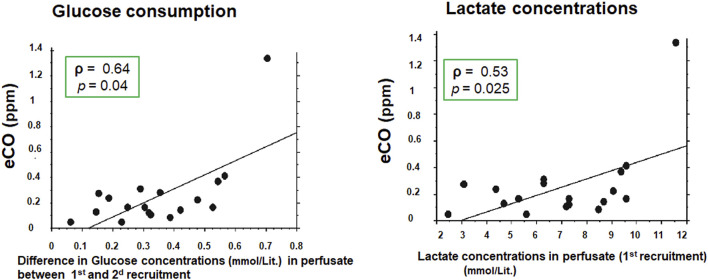
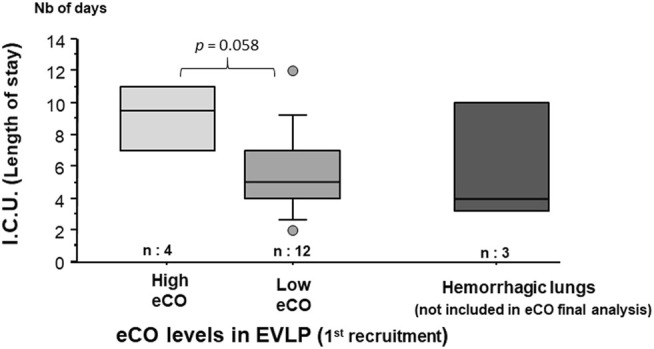
Endogenous production of carbon monoxide (CO) is affected by inflammatory phenomena and ischemia-reperfusion injury. Precise measurement of exhaled endogenous CO (eCO) is possible thanks to a laser spectrometer (ProCeas® from AP2E company). We assessed eCO levels of human lung grafts during the normothermic Ex-Vivo Lung Perfusion (EVLP). ProCeas® was connected in bypass to the ventilation circuit. The surgical team took the decision to transplant the lungs without knowing eCO values. We compared eCO between accepted and rejected grafts. EVLP parameters and recipient outcomes were also compared with eCO values. Over 7 months, eCO was analyzed in 21 consecutive EVLP grafts. Two pairs of lungs were rejected by the surgical team. In these two cases, there was a tendency for higher eCO values (0.358 ± 0.52 ppm) compared to transplanted lungs (0.240 ± 0.76 ppm). During the EVLP procedure, eCO was correlated with glucose consumption and lactate production. However, there was no association of eCO neither with edema formation nor with the PO2/FiO2 ratio per EVLP. Regarding post-operative data, every patient transplanted with grafts exhaling high eCO levels (>0.235 ppm) during EVLP presented a Primary Graft Dysfunction score of 3 within the 72 h post-transplantation. There was also a tendency for a longer stay in ICU for recipients with grafts exhaling high eCO levels during EVLP. eCO can be continuously monitored during EVLP. It could serve as an additional and early marker in the evaluation of the lung grafts providing relevant information for post-operative resuscitation care.
Keywords: carbon monoxide; cavity enhanced laser absorption spectroscopy; ex-vivo lung perfusion; gasotransmitters; ischemia-reperfusion; lung inflammation; lung transplant; spectroscopy.
Copyright © 2022 Brenckmann, Briot, Ventrillard, Romanini, Barbado, Jaulin, Trocme, De Wolf, Glorion and Sage.
Conflict of interest statement
Author KJ was employed by the company AP2E Company. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Snell GI, Yusen RD, Weill D, Strueber M, Garrity E, Reed A, et al. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction, Part I: Definition and Grading-A 2016 Consensus Group Statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant (2017) 36(10):1097–103. 10.1016/j.healun.2017.07.021 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical