

Additive Impact of Interleukin 6 and Neuron Specific Enolase for Prognosis in Patients With Out-of-Hospital Cardiac Arrest - Experience From the HAnnover COoling REgistry
- PMID: 35711345
- PMCID: PMC9194609
- DOI: 10.3389/fcvm.2022.899583
Additive Impact of Interleukin 6 and Neuron Specific Enolase for Prognosis in Patients With Out-of-Hospital Cardiac Arrest - Experience From the HAnnover COoling REgistry
Abstract
Background: Patients after out-of-hospital cardiac arrest (OHCA) are at increased risk for mortality and poor neurological outcome. We assessed the additive impact of interleukin 6 (IL-6) at admission to neuron-specific enolase (NSE) at day 3 for prognosis of 30-day mortality and long-term neurological outcome in OHCA patients.
Methods: A total of 217 patients from the HAnnover COoling REgistry with return of spontaneous circulation (ROSC) after OHCA and IL-6 measurement immediately after admission during 2017-2020 were included to investigate the prognostic value and importance of IL-6 in addition to NSE obtained on day 3. Poor neurological outcome was defined by cerebral performance category (CPC) ≥ 3 after 6 months.
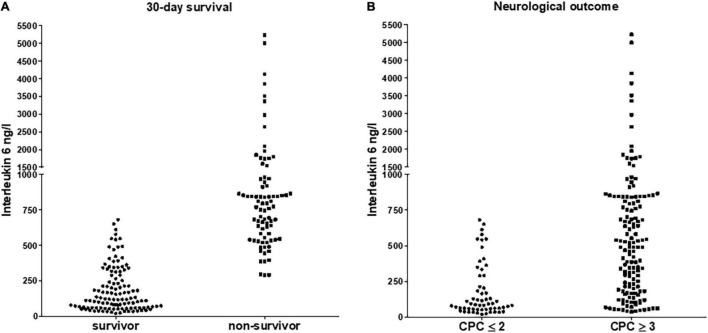
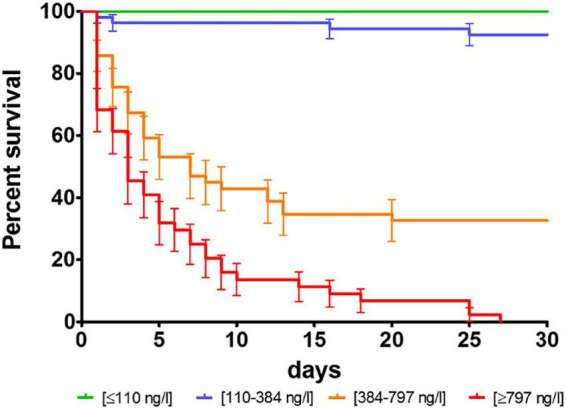
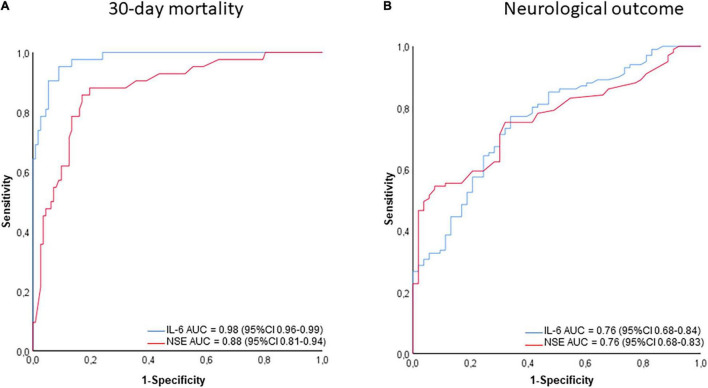
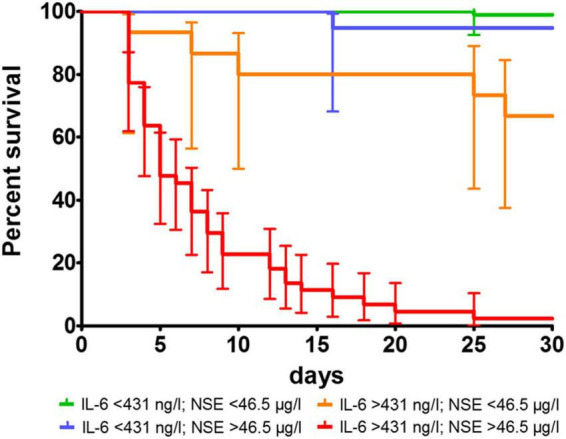
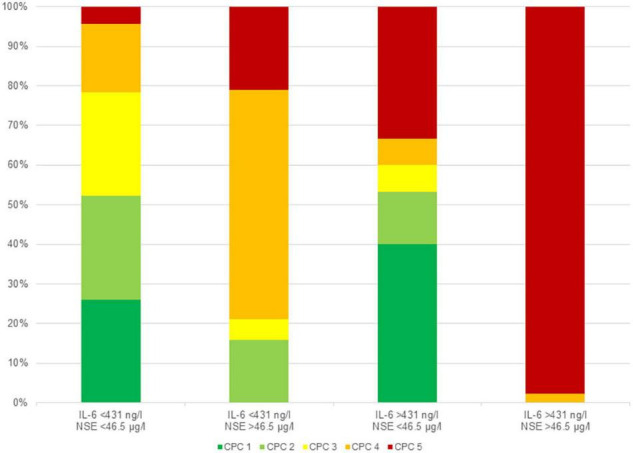
Results: Patients with poor outcome showed higher IL-6 values (30-day mortality: 2,224 ± 524 ng/l vs 186 ± 15 ng/l, p < 0.001; CPC ≥ 3 at 6 months: 1,440 ± 331 ng/l vs 180 ± 24 ng/l, p < 0.001). IL-6 was an independent predictor of mortality (HR = 1.013/ng/l; 95% CI 1.007-1.019; p < 0.001) and poor neurological outcome (HR = 1.004/ng/l; 95% CI 1.001-1.007; p = 0.036). In ROC-analysis, AUC for IL-6 was 0.98 (95% CI 0.96-0.99) for mortality, but only 0.76 (95% CI 0.68-0.84) for poor neurological outcome. The determined cut-off value for IL-6 was 431 ng/l for mortality (NPV 89.2%). In patients with IL-6 > 431 ng/l, the combination with NSE < 46 μg/l optimally identified those individuals with potential for good neurological outcome (CPC ≤ 2).
Conclusion: Elevated IL-6 levels at admission after ROSC were closely associated with 30-day mortality. The combination of IL-6 and NSE provided clinically important additive information for predict poor neurological outcome at 6 months.
Keywords: interleukin 6; neurological outcome; neuron-specific enolase; out-of-hospital cardiac arrest; prognosis.
Copyright © 2022 Akin, Sieweke, Garcheva, Martinez, Adel, Plank, Zandian, Sühs, Bauersachs and Schäfer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Neuromarkers and neurological outcome in out-of-hospital cardiac arrest patients treated with therapeutic hypothermia-experience from the HAnnover COoling REgistry (HACORE).PLoS One. 2021 Jan 7;16(1):e0245210. doi: 10.1371/journal.pone.0245210. eCollection 2021. PLoS One. 2021. PMID: 33411836 Free PMC article. Clinical Trial.
-
Serum neuron-specific enolase as predictor of outcome in comatose cardiac-arrest survivors: a prospective cohort study.BMC Cardiovasc Disord. 2011 Aug 8;11:48. doi: 10.1186/1471-2261-11-48. BMC Cardiovasc Disord. 2011. PMID: 21824428 Free PMC article.
-
Neuron-specific enolase kinetics: an additional tool for neurological prognostication after cardiac arrest.Rev Esp Cardiol (Engl Ed). 2020 Feb;73(2):123-130. doi: 10.1016/j.rec.2019.01.008. Epub 2019 Mar 8. Rev Esp Cardiol (Engl Ed). 2020. PMID: 30857978 English, Spanish.
-
Association of neuron-specific enolase values with outcomes in cardiac arrest survivors is dependent on the time of sample collection.Crit Care. 2017 Jul 8;21(1):172. doi: 10.1186/s13054-017-1766-2. Crit Care. 2017. PMID: 28687073 Free PMC article.
-
Admission interleukin-6 is associated with post resuscitation organ dysfunction and predicts long-term neurological outcome after out-of-hospital ventricular fibrillation.Resuscitation. 2014 Nov;85(11):1573-9. doi: 10.1016/j.resuscitation.2014.08.036. Epub 2014 Sep 17. Resuscitation. 2014. PMID: 25238742
Cited by
-
Predictive Performance of Neuron-Specific Enolase (NSE) for Survival after Resuscitation from Cardiac Arrest: A Systematic Review and Meta-Analysis.J Clin Med. 2023 Dec 13;12(24):7655. doi: 10.3390/jcm12247655. J Clin Med. 2023. PMID: 38137724 Free PMC article. Review.
-
Neutrophil to high-density lipoprotein cholesterol ratio as a potential inflammatory marker for predicting all-cause mortality in out-of-hospital cardiac arrest survivors.Sci Rep. 2025 May 17;15(1):17181. doi: 10.1038/s41598-025-01951-x. Sci Rep. 2025. PMID: 40382458 Free PMC article.
-
Cytokine hemoadsorption with CytoSorb® in post-cardiac arrest syndrome, a pilot randomized controlled trial.Crit Care. 2023 Jan 23;27(1):36. doi: 10.1186/s13054-023-04323-x. Crit Care. 2023. PMID: 36691082 Free PMC article. Clinical Trial.
References
-
- Ruhfus M, Giannakis S, Markus M, Stein A, Hoehn T, Felderhoff-Mueser U, et al. Association of routinely measured proinflammatory biomarkers with abnormal MRI findings in asphyxiated neonates undergoing therapeutic hypothermia. Front Pediatr. (2021) 9:624652. 10.3389/fped.2021.624652 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous