

The Preperitoneal Space in Hernia Repair
- PMID: 35711709
- PMCID: PMC9197412
- DOI: 10.3389/fsurg.2022.869731
The Preperitoneal Space in Hernia Repair
Abstract
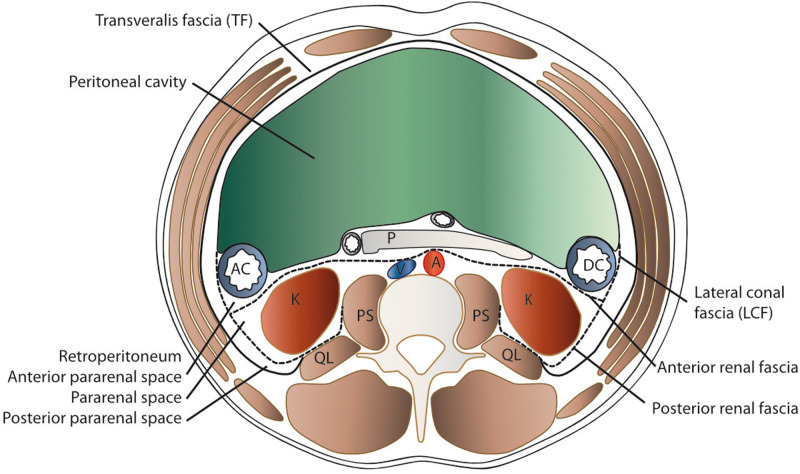
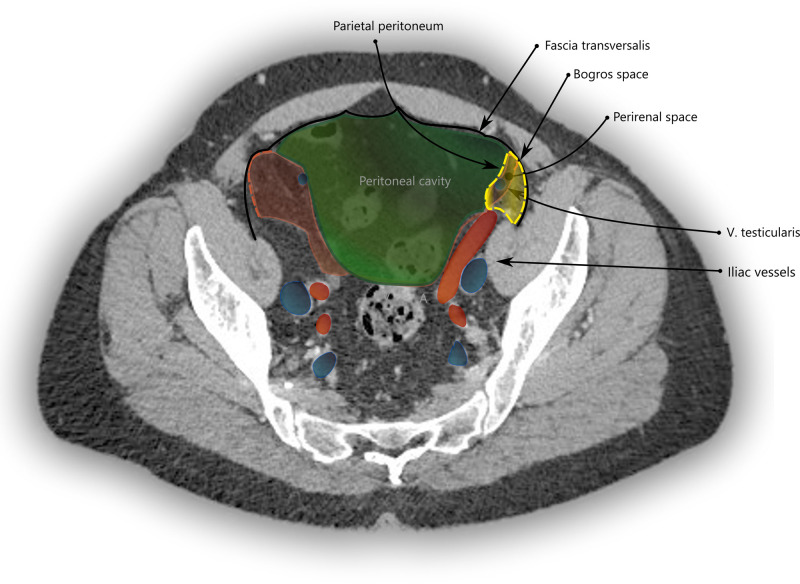
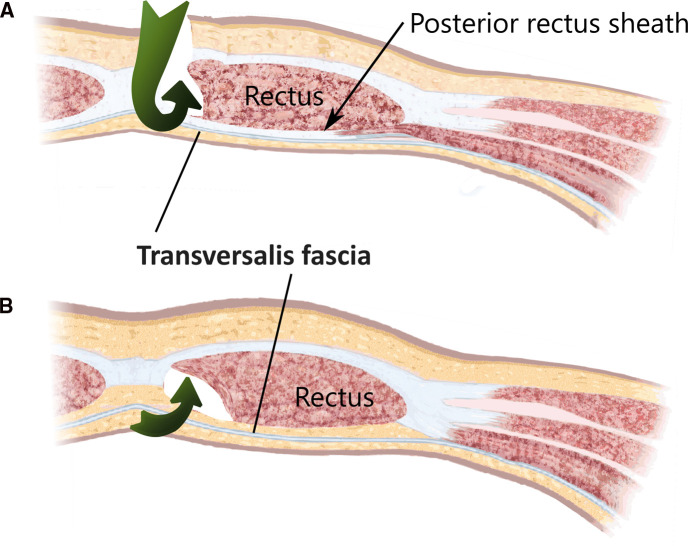
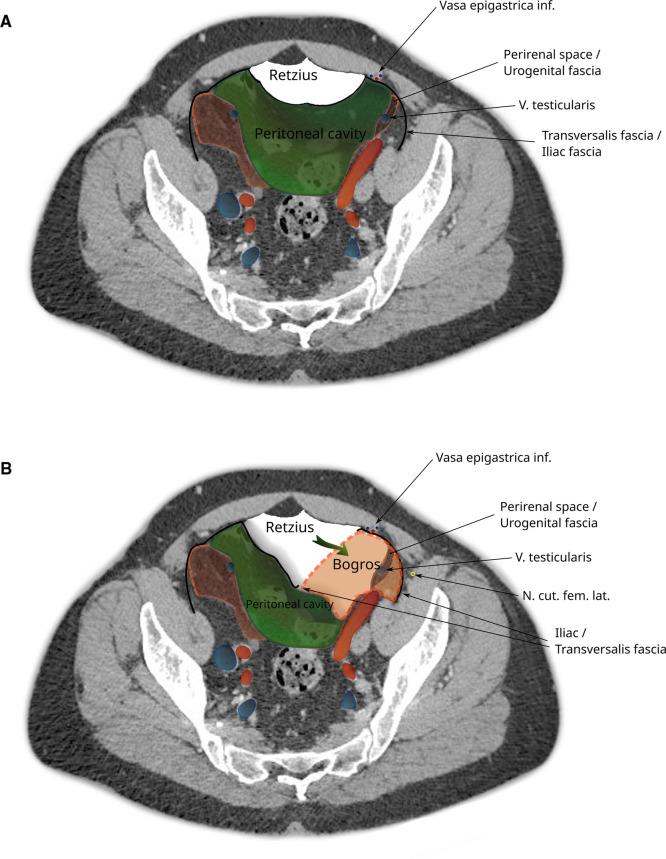
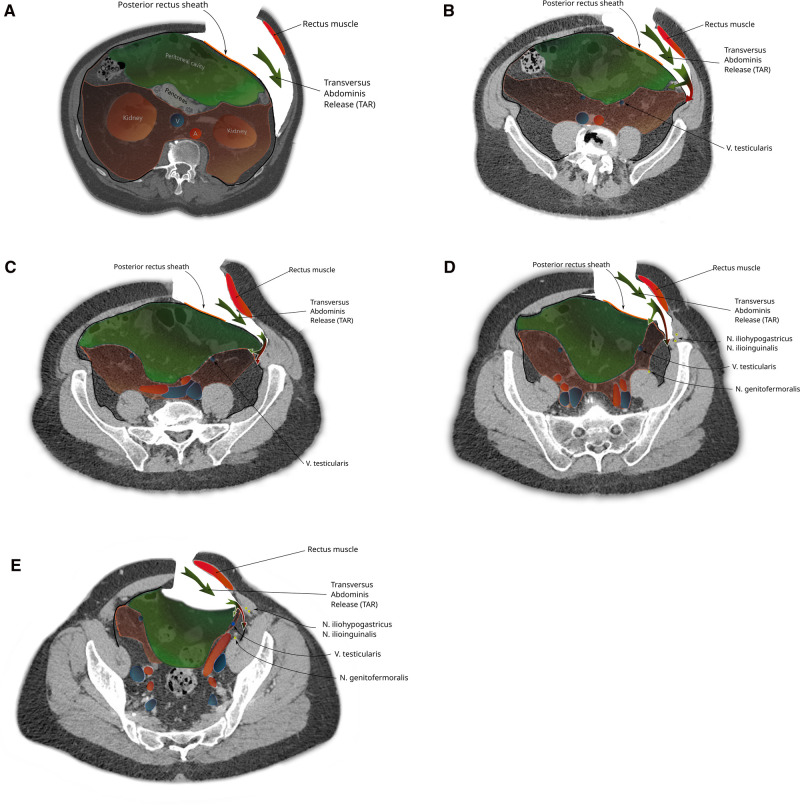
The preperitoneal spaces relevant for incisional hernia repair and minimally invasive groin hernia repair are described in terms of surgical anatomy. Emphasis is put on the transversalis fascia and the urogenital fascia and its extensions, the vesicoumbilical fascia, and the spermatic sheath of Stoppa procedure. Steps in hernia surgery where these structures are relevant are reviewed.
Keywords: abdominal wall repair; anatomy; groin hernia; retroperitoneum; transversalis fascia.
Copyright © 2022 Lorenz, Augustin, Konschake, Gehwolf, Henninger, Augustin and Öfner.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Cooper AP. The anatomy and surgical treatment of inguinal and congential hernia. London, United Kingdom (1804).
-
- Cruveilhier J. The anatomy of the human body. New York: Harper & Brothers; (1844). 305 p.
-
- Mackay JY. The relations of the aponeurosis of the transversalis and internal oblique muscles to the deep epigastric artery and to the inguinal canal. In: Cleland J, Mackay JY, Young RB, editors. Memoirs and memoranda in anatomy, Vol. I. London: Williams and Norgate; (1889). p. 143–5.
-
- McVay C, Anson BJ. Composition of the rectus sheath. Anat Rec. (1940) 77:213–25. 10.1002/ar.1090770210 - DOI
-
- Lytle WJ. The internal inguinal ring. Br J Surg. (1945) 32:441–6. 10.1002/bjs.18003212802 - DOI
Publication types
LinkOut - more resources
Full Text Sources