

Evidence on Indications and Techniques to Increase the Future Liver Remnant in Children Undergoing Extended Hepatectomy: A Systematic Review and Meta-Analysis of Individual Patient Data
- PMID: 35712634
- PMCID: PMC9197416
- DOI: 10.3389/fped.2022.915642
Evidence on Indications and Techniques to Increase the Future Liver Remnant in Children Undergoing Extended Hepatectomy: A Systematic Review and Meta-Analysis of Individual Patient Data
Abstract
Background: Techniques to increase the future liver remnant (FLR) have fundamentally changed the indications and criteria of resectability in adult liver surgery. In pediatric patients however, these procedures have rarely been applied and the potential benefit or harm as well as suited indications are unclear.
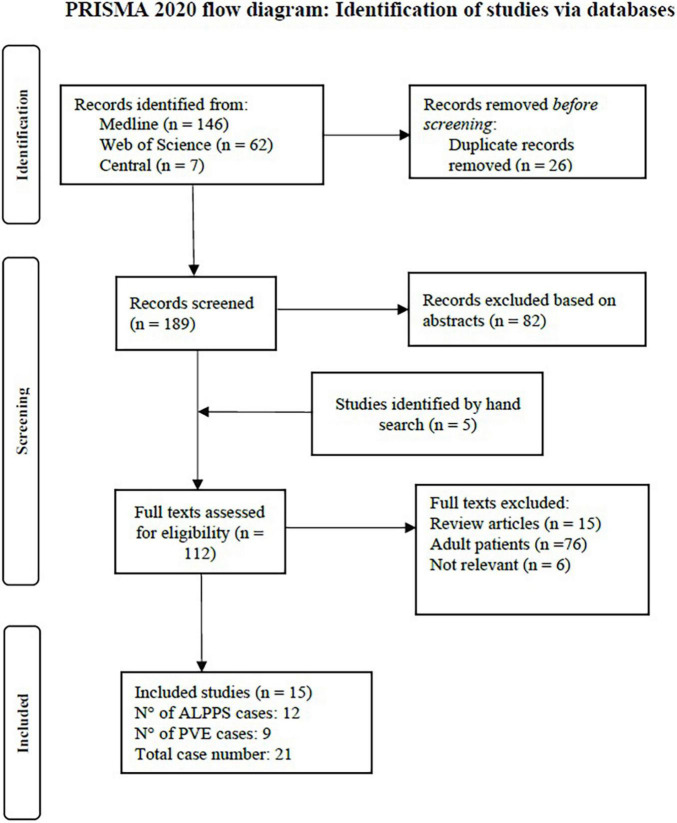
Methods: A systematic literature search of MEDLINE, Web of Science, and CENTRAL was conducted. Based on a PRISMA-compliant, predefined methodology, all studies reporting pediatric patients (< 18y) undergoing liver resection with either associating liver partition and portal vein ligation for stages hepatectomy (ALPPS) or preoperative portal vein embolization or ligation (PVE/PVL) were included. Baseline data, periinterventional morbidity, increase of FLR and outcomes were analyzed.
Results: 15 studies reporting on 21 pediatric patients with a mean age of 4 years and 7 months (range 1.8 months - 17 years) were included. 12 ALPPS procedures, 8 PVE and 1 PVL were performed. The applied criteria for performing ALPPS or PVE were heterogenous and thresholds for minimally acceptable FLR varied. Mean FLR [% of total liver volume] before the intervention was 23.6% (range 15.0 - 39.3%) in the ALPPS group and 31.4% (range 21.5 - 56.0%) in the PVE group. Mean increase of FLR before stage 2 resection was 69.4% (range 19.0 - 103.8%) for ALPPS and 62.8% (range 25.0 - 108.0%) after PVE. No postoperative death occurred, one early intrahepatic recurrence after an ALPPS procedure was reported. Overall postoperative morbidity was 23.8%.
Conclusion: Validated criteria for minimal FLR in pediatric liver resection are lacking and so are clear indications for ALPPS or PVE. In special cases, ALPPS and PVE can be valuable techniques to achieve complete resection of pediatric liver tumors. However, more data are needed, and future studies should focus on a definition and validation of posthepatectomy liver failure as well as the minimally needed FLR in pediatric patients undergoing extended hepatectomy.
Systematic review registration: [www.clinicaltrials.gov], identifier [PROSPERO 2021 CRD42021274848].
Keywords: ALPPS; pediatric liver resection; pediatric liver surgery; pediatric liver tumors; pediatric surgery; portal vein embolization.
Copyright © 2022 Fuchs, Murtha-Lemekhova, Rabaux-Eygasier, Kessler, Ruping, Günther and Hoffmann.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Ng K, Mogul DB. Pediatric liver tumors. Clin Liver Dis. (2018) 22: 753–72. - PubMed
-
- Tucker O, Heaton N. The ‘small for size’liver syndrome. Curr Opin Critic Care. (2005) 11:150–5. - PubMed
-
- Søreide JA, Deshpande R. Post Hepatectomy Liver Failure (PHLF)–Recent advances in prevention and clinical management. Eur J Surg Oncol. (2021) 47:216–24. - PubMed
Publication types
LinkOut - more resources
Full Text Sources