

Interleukin-6 Predicts Carotid Plaque Severity, Vulnerability, and Progression
- PMID: 35713008
- PMCID: PMC9308732
- DOI: 10.1161/CIRCRESAHA.122.320877
Interleukin-6 Predicts Carotid Plaque Severity, Vulnerability, and Progression
Abstract
Background: IL-6 (interleukin-6) has important roles in atherosclerosis pathophysiology. To determine if anti-IL-6 therapy warrants evaluation as an adjuvant stroke prevention strategy in patients with carotid atherosclerosis, we tested whether circulating IL-6 levels predict carotid plaque severity, vulnerability, and progression in the prospective population-based CHS (Cardiovascular Health Study).
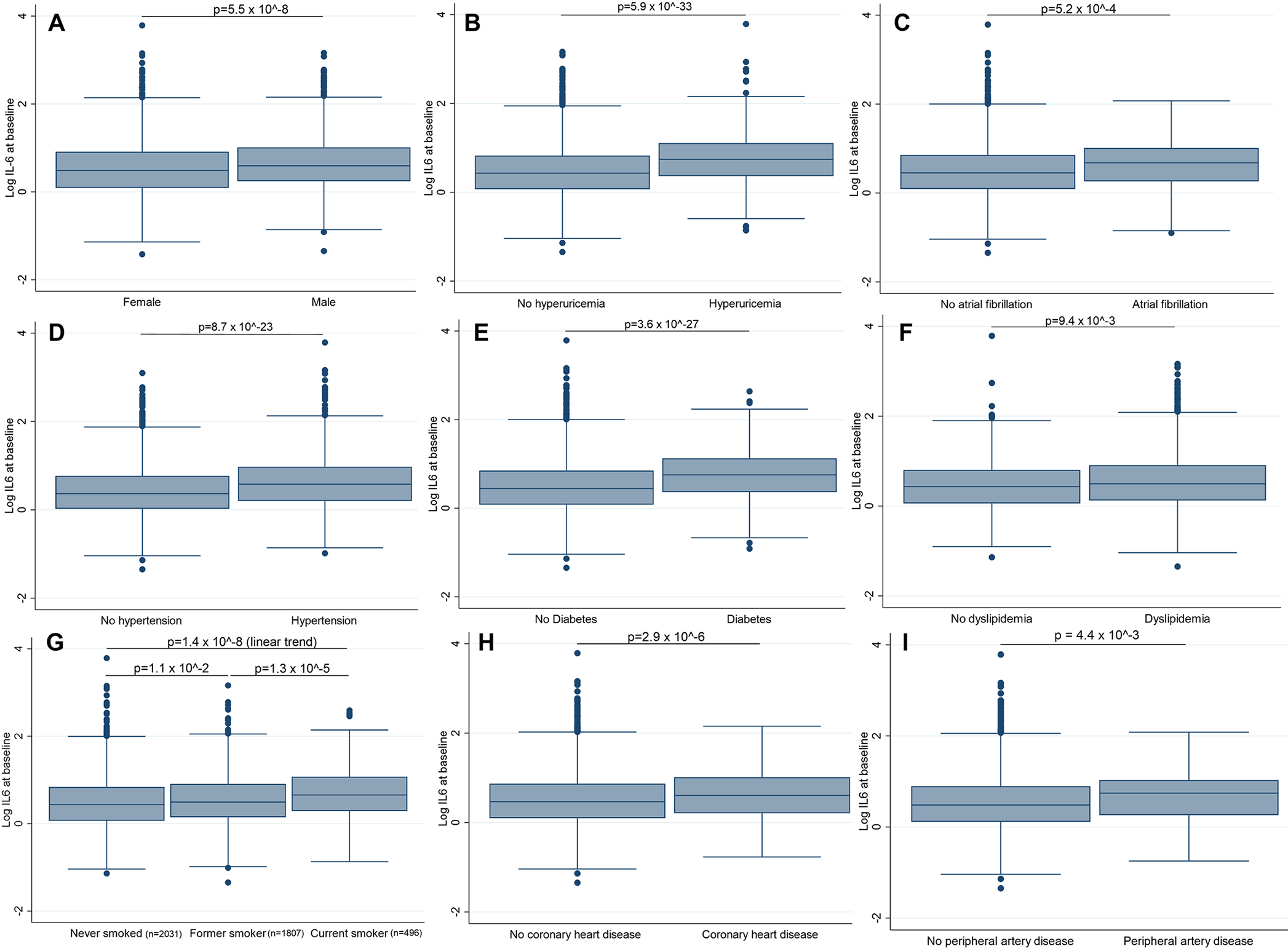
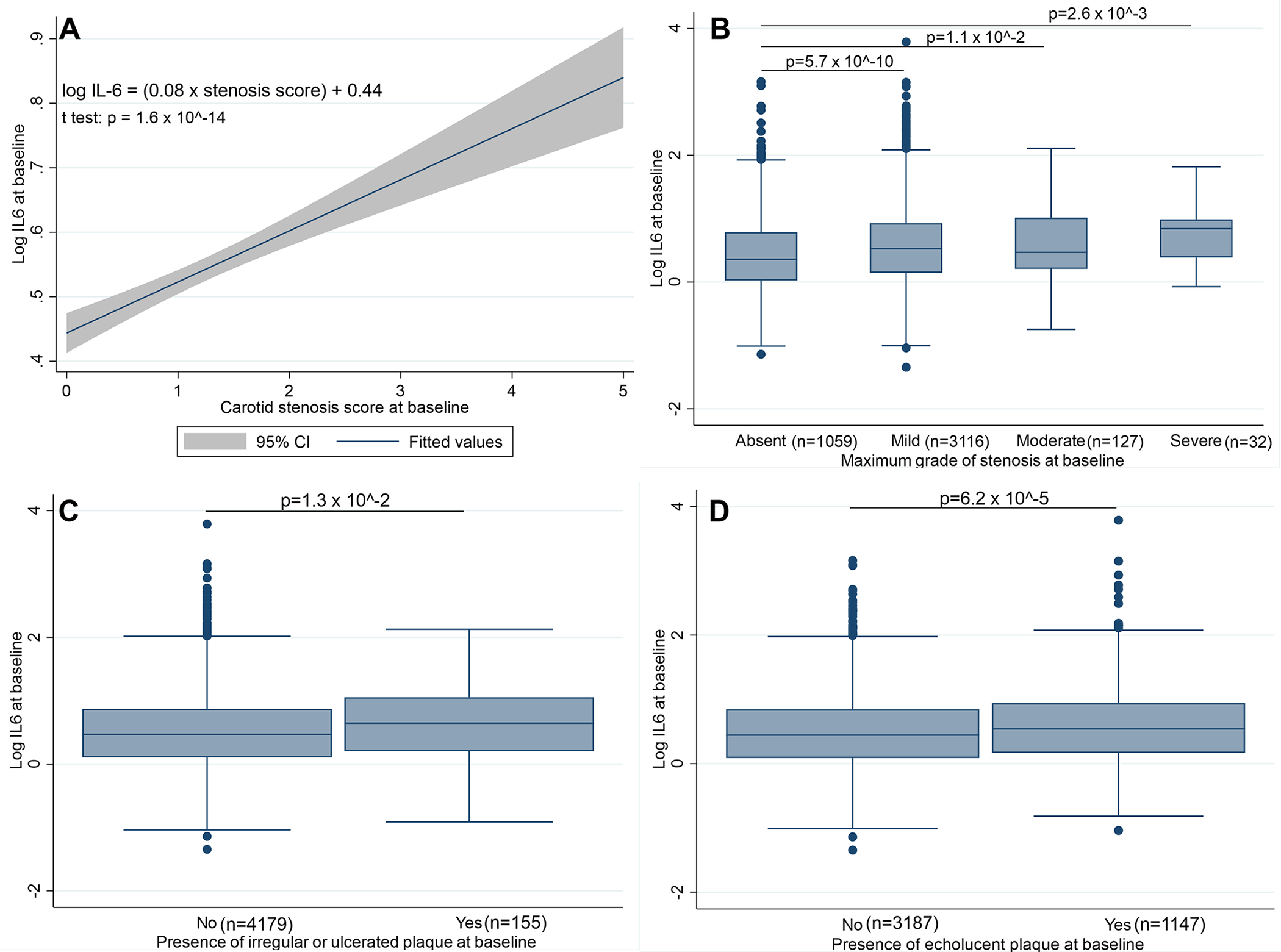
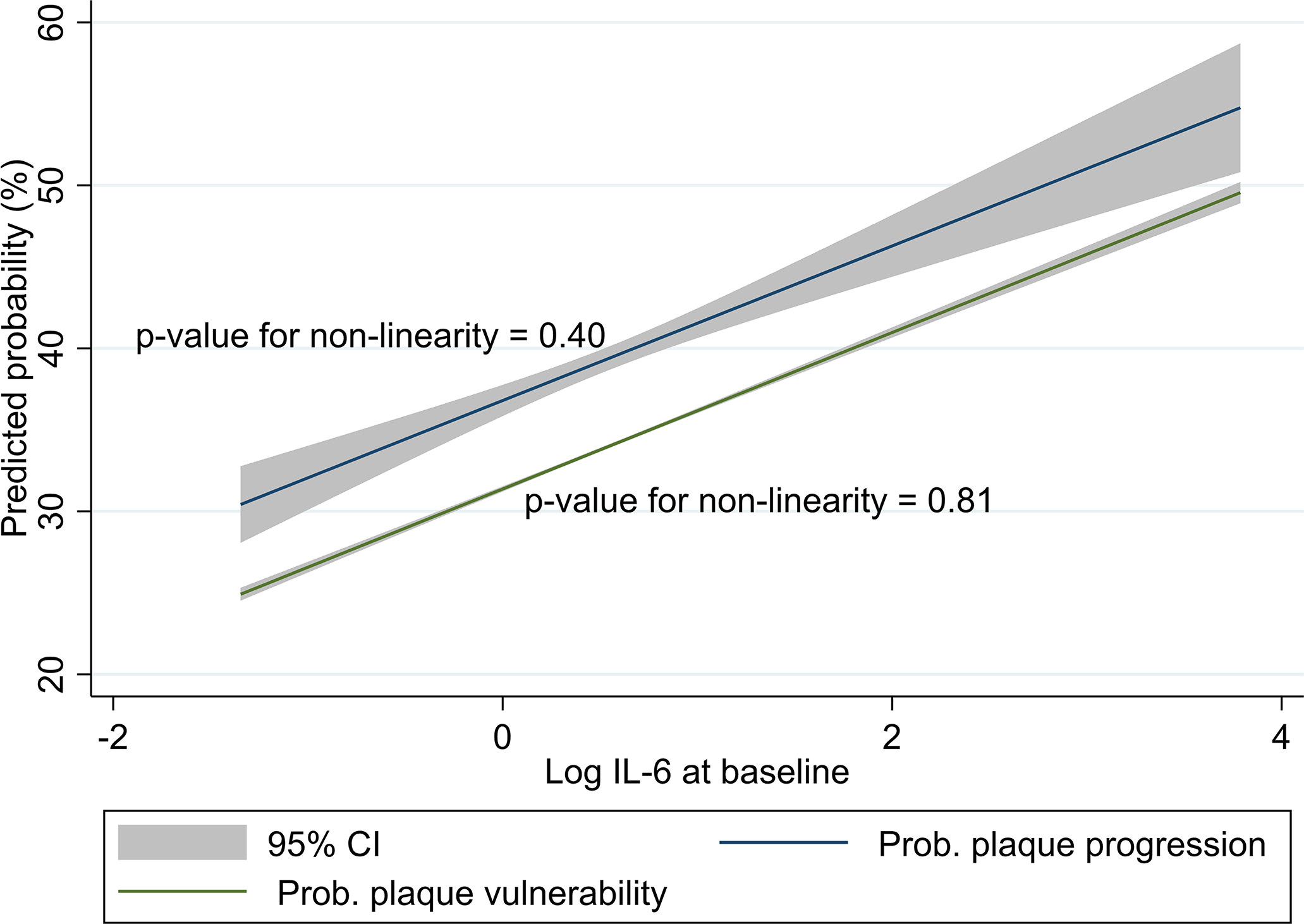
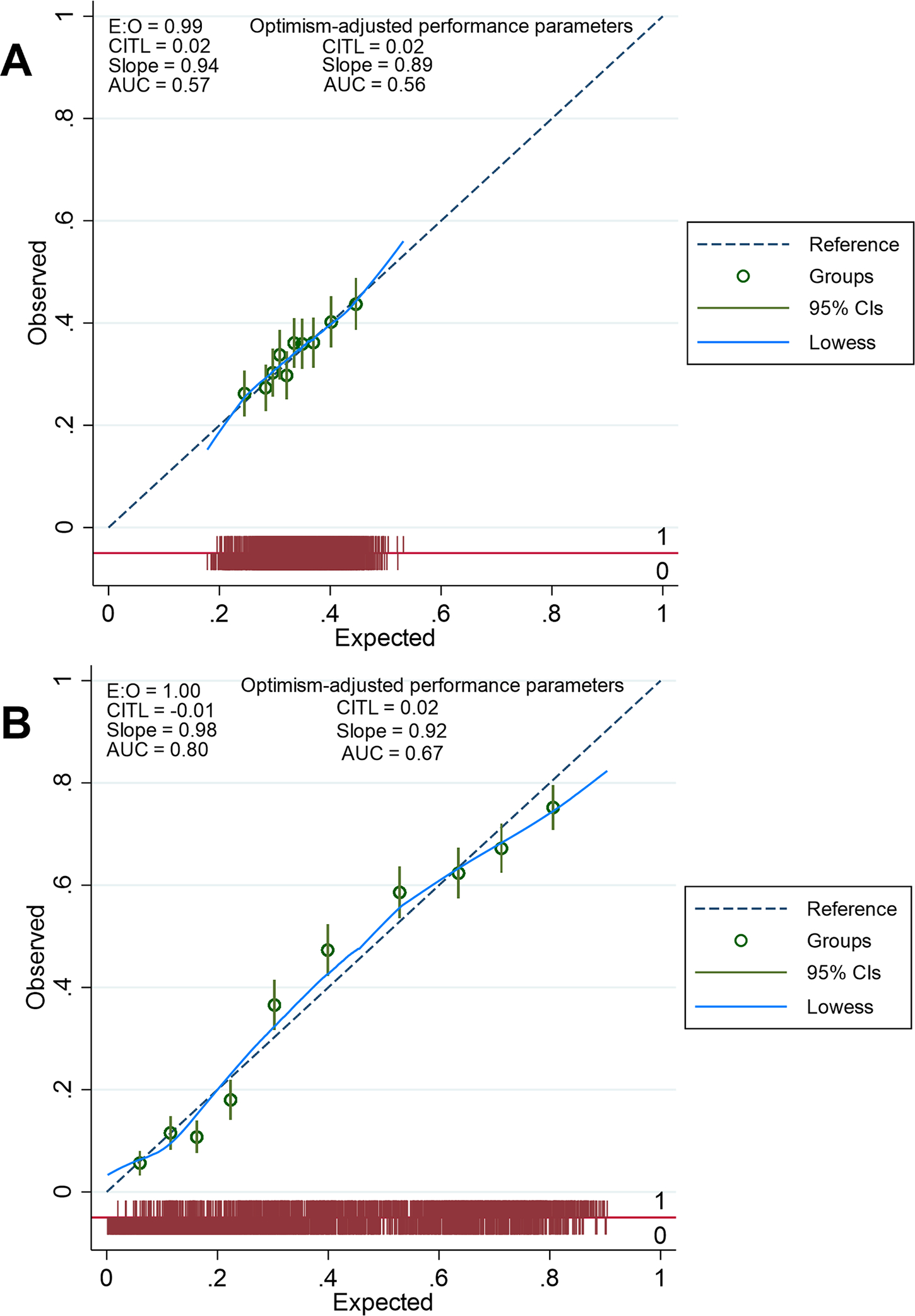
Methods: Duplex carotid ultrasound was performed at baseline and 5 years. Baseline plaque severity was scored 0 to 5 based on North American Symptomatic Carotid Endarterectomy Trial grade of stenosis. Plaque vulnerability at baseline was the presence of markedly irregular, ulcerated, or echolucent plaques. Plaque progression at 5 years was a ≥1 point increase in stenosis severity. The relationship of baseline plasma IL-6 levels with plaque characteristics was modeled using multivariable linear (severity) or logistic (vulnerability and progression) regression. Risk factors of atherosclerosis were included as independent variables. Stepwise backward elimination was used with P>0.05 for variable removal. To assess model stability, we computed the E-value or minimum strength of association (odds ratio scale) that unmeasured confounders must have with log IL-6 and the outcome to suppress the association. We performed internal validation with 100 bootstrap samples.
Results: There were 4334 participants with complete data (58.9% women, mean age: 72.7±5.1 years), including 1267 (29.2%) with vulnerable plaque and 1474 (34.0%) with plaque progression. Log IL-6 predicted plaque severity (β=0.09, P=1.3×10-3), vulnerability (OR, 1.21 [95% CI, 1.05-1.40]; P=7.4×10-3, E-value=1.71), and progression (OR, 1.44 [95% CI, 1.23-1.69], P=9.1×10-6, E-value 2.24). In participants with >50% predicted probability of progression, mean log IL-6 was 0.54 corresponding to 2.0 pg/mL. Dichotomizing IL-6 levels did not affect the performance of prediction models.
Conclusions: Circulating IL-6 predicts carotid plaque severity, vulnerability, and progression. The 2.0 pg/mL cutoff could facilitate the selection of individuals that would benefit from anti-IL-6 drugs for stroke prevention.
Trial registration: ClinicalTrials.gov NCT02089217.
Keywords: atherosclerosis; carotid stenosis; inflammation; interleukin-6; stroke.
Conflict of interest statement
Disclosures
Joseph Kamtchum-Tatuene was funded by the Faculty of Graduate Studies and Research Doctoral Recruitment Scholarship, the Bank of Montreal Graduate Scholarship, the Alberta Graduate Excellence Scholarship, the Faculty of Medicine and Dentistry Motyl Graduate Studentship in Cardiac Sciences, the Alberta Innovates Graduate Scholarship, the Department of Medicine Ballermann Translational Research Fellowship, the Izaak Walton Killam Memorial Scholarship, and the Andrew Stewart Memorial Graduate Prize. All awards, prizes, and scholarships managed by the University of Alberta.
Luca Saba reports no conflicts of interest.
Mirjam R. Heldner reports grants from the Swiss Heart Foundation and the Bangerter Foundation, and Advisory Board participation for Amgen.
Michiel H. F. Poorthuis reports no conflicts of interest.
Gert J. de Borst reports no conflicts of interest.
Tatjana Rundek is funded by grants from the National Institutes of Health (R01 NS040807, R01 NS029993, R01 MD012467, RF1AG074306, U24 NS107267, P30 AG066506, HHSN268200625234C, U19 AG056169), the National Center for Advancing Translational Sciences (UL1 TR002736, KL2 TR002737), and the Florida Department of Health.
Stavros K. Kakkos reports no conflicts of interest.
Seemant Chaturvedi serves on the Executive Committee of the Carotid Revascularization and Medical Management for Asymptomatic Carotid Stenosis Trial (CREST-2,
Raffi Topakian has received fees for serving as Advisory Board Member (Alexion, Roche, Sanofi-Aventis) and conference support from the industry (Daiichi-Sankyo, Pfizer, Roche), all within the last three years.
Joseph F. Polak reports no conflicts of interest.
Glen C. Jickling receives research grant support from Canadian Institutes of Health Research (CIHR), Heart and Stroke Foundation, Alberta University Hospital Foundation, Canada Foundation for Innovation (CFI), and National Institutes of Health (NIH).
Figures
References
-
- Libby P, Buring JE, Badimon L, Hansson GK, Deanfield J, Bittencourt MS, Tokgozoglu L, Lewis EF. Atherosclerosis. Nat Rev Dis Primers. 2019;5:56. - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2018;49:e46–e110. - PubMed
-
- Ridker PM, Everett BM, Thuren T, MacFadyen JG, Chang WH, Ballantyne C, Fonseca F, Nicolau J, Koenig W, Anker SD, et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N Engl J Med. 2017;377:1119–1131. - PubMed
-
- Ridker PM, Libby P, MacFadyen JG, Thuren T, Ballantyne C, Fonseca F, Koenig W, Shimokawa H, Everett BM, Glynn RJ. Modulation of the interleukin-6 signalling pathway and incidence rates of atherosclerotic events and all-cause mortality: analyses from the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS). Eur Heart J. 2018;39:3499–3507. - PubMed
-
- Ridker PM, MacFadyen JG, Thuren T, Libby P. Residual inflammatory risk associated with interleukin-18 and interleukin-6 after successful interleukin-1beta inhibition with canakinumab: further rationale for the development of targeted anti-cytokine therapies for the treatment of atherothrombosis. Eur Heart J. 2020;41:2153–2163. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- RF1 AG074306/AG/NIA NIH HHS/United States
- U24 NS107267/NS/NINDS NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- N01 HC085085/HC/NHLBI NIH HHS/United States
- R01 MD012467/MD/NIMHD NIH HHS/United States
- R01 NS040807/NS/NINDS NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- R01 NS029993/NS/NINDS NIH HHS/United States
- 75N92021D00006/HL/NHLBI NIH HHS/United States
- P30 AG066506/AG/NIA NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- N01 HC085080/HL/NHLBI NIH HHS/United States
- R56 AG056169/AG/NIA NIH HHS/United States
- KL2 TR002737/TR/NCATS NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- UL1 TR002736/TR/NCATS NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- R01 AG056169/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
