

Immune enhancement in patients with predicted severe acute necrotising pancreatitis: a multicentre double-blind randomised controlled trial
- PMID: 35713670
- PMCID: PMC9205279
- DOI: 10.1007/s00134-022-06745-7
Immune enhancement in patients with predicted severe acute necrotising pancreatitis: a multicentre double-blind randomised controlled trial
Abstract
Purpose: Infected pancreatic necrosis (IPN) is a highly morbid complication of acute necrotising pancreatitis (ANP). Since there is evidence of early-onset immunosuppression in acute pancreatitis, immune enhancement may be a therapeutic option. This trial aimed to evaluate whether early immune-enhancing Thymosin alpha 1 (Tα1) treatment reduces the incidence of IPN in patients with predicted severe ANP.
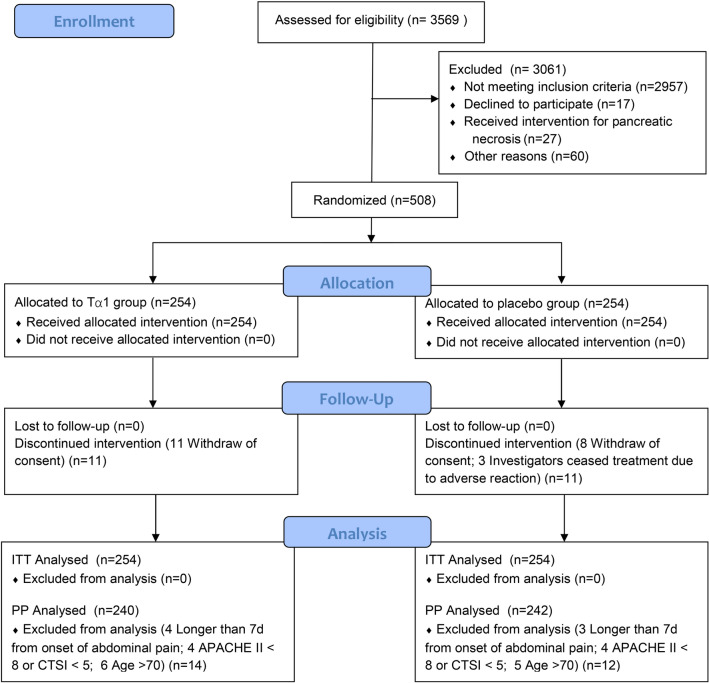
Methods: We conducted a multicentre, double-blind, randomised, placebo-controlled trial involving ANP patients with an Acute Physiology and Chronic Health Evaluation II (APACHE II) score ≥ 8 and a computed tomography (CT) severity score ≥ 5 admitted within 7 days of the advent of symptoms. Enrolled patients were assigned to receive a subcutaneous injection of Tα1 1.6 mg every 12 h for the first 7 days and 1.6 mg once a day for the subsequent 7 days or matching placebos (normal saline). The primary outcome was the development of IPN during the index admission.
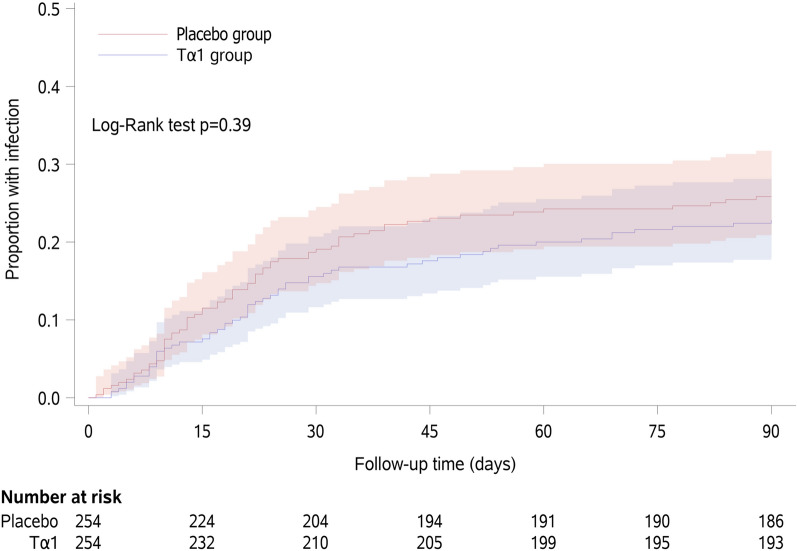
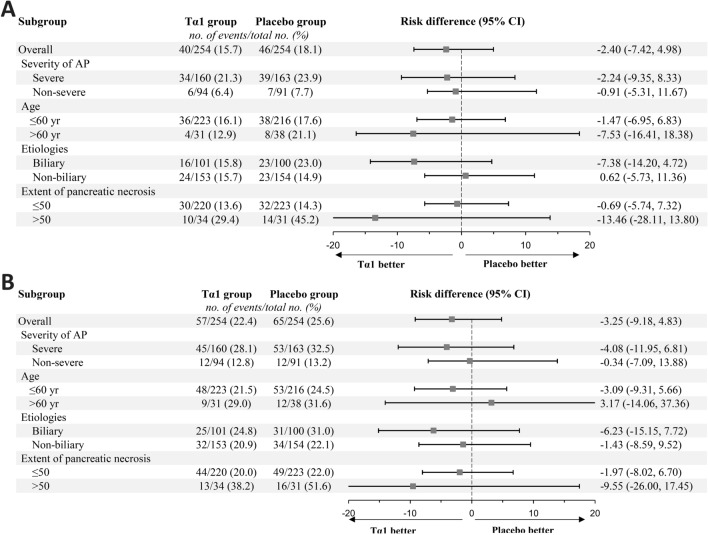
Results: A total of 508 patients were randomised, of whom 254 were assigned to receive Tα1 and 254 placebo. The vast majority of the participants required admission to the intensive care unit (ICU) (479/508, 94.3%). During the index admission, 40/254(15.7%) patients in the Tα1 group developed IPN compared with 46/254 patients (18.1%) in the placebo group (difference -2.4% [95% CI - 7.4 to 5.1%]; p = 0.48). The results were similar across four predefined subgroups. There was no difference in other major complications, including new-onset organ failure (10.6% vs. 15%), bleeding (6.3% vs. 3.5%), and gastrointestinal fistula (2% vs. 2.4%).
Conclusion: The immune-enhancing Tα1 treatment of patients with predicted severe ANP did not reduce the incidence of IPN during the index admission.
Keywords: Acute pancreatitis; Immunosuppression; Infection; Pancreatic necrosis; Thymosin.
© 2022. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
WL reports consultancy fees and grants from SciClone Pharmaceuticals. ZT reports speaker fees from SciClone Pharmaceuticals. LK reports speaker fees from SciClone Pharmaceuticals. VS reports consultant fees and grants Abbvie, medical advisory board participant for Envara, and grants from Theraly and Orgenesis. The other authors have no relevant conflict of interest to declare.
Figures
Comment in
-
Immune Enhancement in Patients With Predicted Severe Acute Necrotizing Pancreatitis: Important Implications for Timing and Early Stratification.Pancreas. 2023 Jul 1;52(6):e344-e346. doi: 10.1097/MPA.0000000000002266. Epub 2023 Nov 10. Pancreas. 2023. PMID: 37944121 No abstract available.
References
-
- Xiao AY, Tan ML, Wu LM, Asrani VM, Windsor JA, Yadav D, Petrov MS. Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol Hepatol. 2016;1:45–55. doi: 10.1016/S2468-1253(16)30004-8. - DOI - PubMed
-
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS, Acute Pancreatitis Classification Working G Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–111. doi: 10.1136/gutjnl-2012-302779. - DOI - PubMed
-
- Trikudanathan G, Wolbrink DRJ, van Santvoort HC, Mallery S, Freeman M, Besselink MG. Current concepts in severe acute and necrotizing pancreatitis: an evidence-based approach. Gastroenterology. 2019;156(1994–2007):e1993. - PubMed
-
- Schepers NJ, Bakker OJ, Besselink MG, Ahmed Ali U, Bollen TL, Gooszen HG, van Santvoort HC, Bruno MJ, Dutch Pancreatitis Study G Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis. Gut. 2019;68:1044–1051. doi: 10.1136/gutjnl-2017-314657. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
