

Management of pericardial tamponade in the electrophysiology laboratory: results from a national survey
- PMID: 35713695
- PMCID: PMC10697891
- DOI: 10.1007/s00392-022-02042-x
Management of pericardial tamponade in the electrophysiology laboratory: results from a national survey
Erratum in
-
Correction to: Management of pericardial tamponade in the electrophysiology laboratory: results from a national survey.Clin Res Cardiol. 2023 Jun;112(6):854. doi: 10.1007/s00392-022-02066-3. Clin Res Cardiol. 2023. PMID: 35925393 Free PMC article. No abstract available.
Abstract
Background: Despite continued efforts to improve the safety of catheter ablation, pericardial tamponade remains one of its more frequent, potentially life-threatening complications. Management of cardiac tamponade is not standardized and uncertainties regarding acute treatment remain.
Methods: This survey sought to evaluate the management of cardiac tamponade in German EP centers via a standardized postal questionnaire. All 341 identified German EP centers were invited to return a questionnaire on their standards for the management of cardiac tamponade.
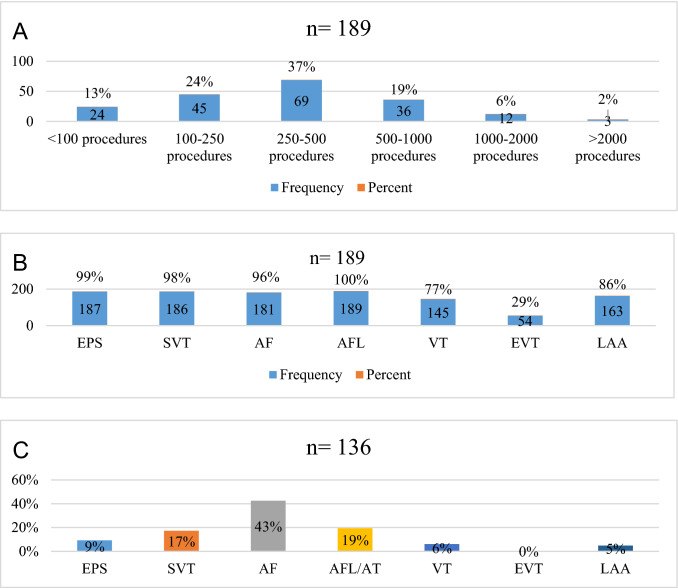
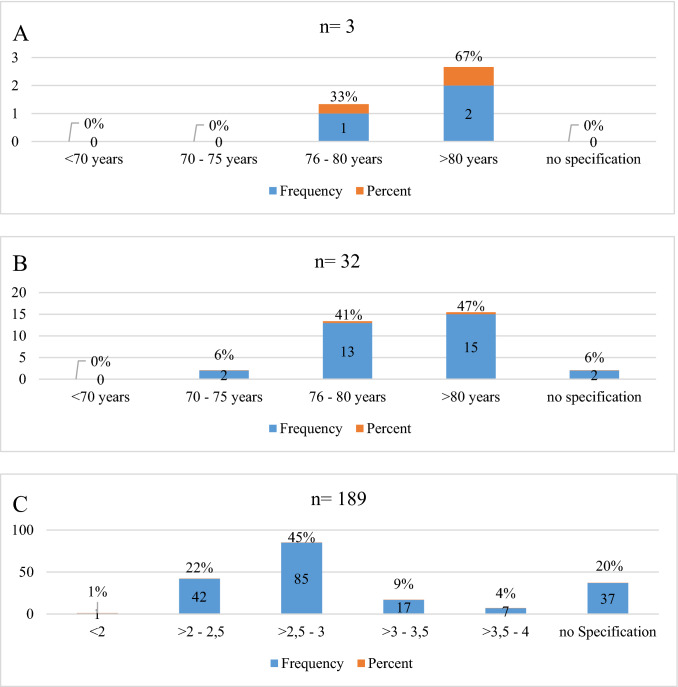
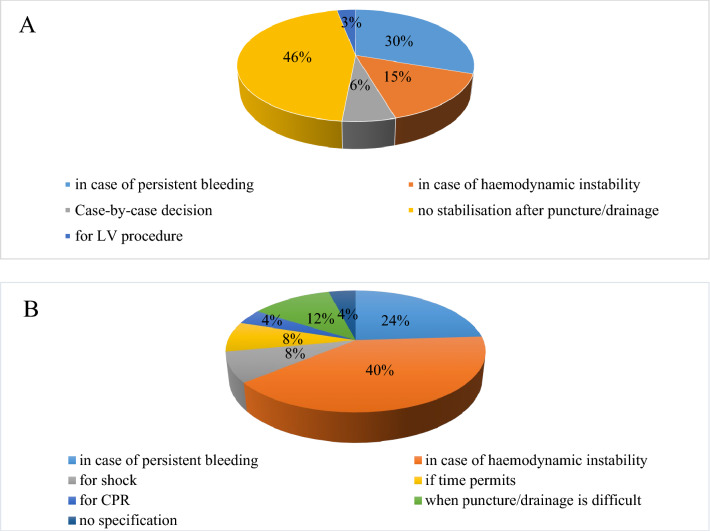
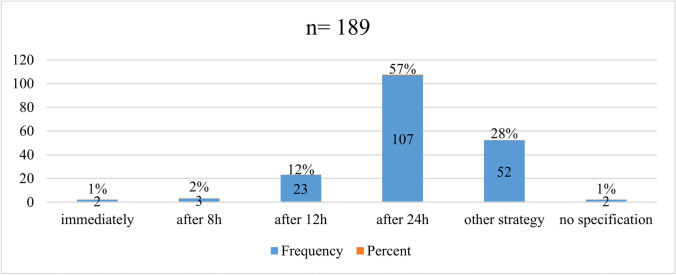
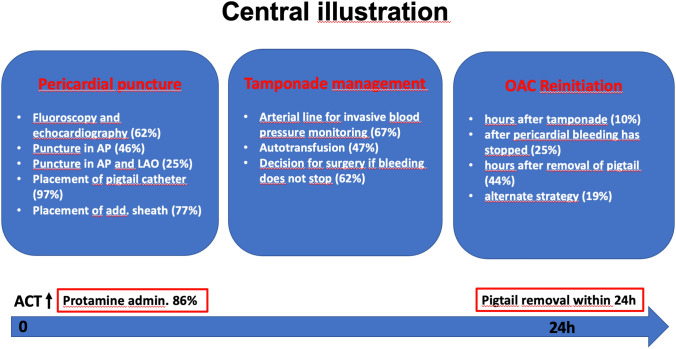
Results: A total of 189 German EP centers completed the questionnaire. Several precautions are followed to avoid pericardial tamponade: A minority of centers preclude very old patients (19%) or those with a high body mass index (30%) from ablation. Non-vitamin K antagonist oral anticoagulants are briefly paused in most centers (88%) before procedures, while vitamin K antagonists are continued. Pericardial tamponade is usually treated using reversal of heparin by applying protamine (86%) and pericardiocentesis under both, fluoroscopic and echocardiographic guidance (62%). A pigtail catheter is mostly inserted (97%) and autotransfusion of aspirated blood is performed in 47% of centers. The decision for surgical repair depends on different clinical and infrastructural aspects. The timing of reinitiation of anticoagulation widely differs between the centers. Approximately 1/3 of centers prescribe nonsteroidal anti-inflammatory agents, colchicine or steroids after pericardiocentesis.
Conclusion: The present survey shows that the management of cardiac tamponade is still inhomogeneous in German ablation centers. However, multiple findings of this survey can be generalized and might guide especially less experienced operators and centers in their treatment and decision strategies.
Keywords: Cardiac tamponade; Catheter ablation; Complication; EP lab; Electrophysiology; Pericardial puncture; Survey.
© 2022. The Author(s).
Conflict of interest statement
Andreas Metzner has received speakers honoraria from Medtronic, Biosense Webster, Boston Scientific and Cardiofocus. Daniel Steven has received speakers honoraria from Abbott, Boston Scientific and Biosense Webster and he received research grants from Medtronic, Abbott and Biosense Webster. Philipp Sommer is Member of the Advisory Board for Abbott, Biosense Webster, Boston Scientific and Medtronic. PK was partially supported by European Union BigData@Heart (grant agreement EU IMI 116074), AFFECT-AF (grant agreement 847770), and MAESTRIA (grant agreement 965286), British Heart Foundation (PG/17/30/32961; PG/20/22/35093; AA/18/2/34218), German Centre for Cardiovascular Research supported by the German Ministry of Education and Research (DZHK), and Leducq Foundation. Paulus Kirchhof receives research support for basic, translational, and clinical research projects from European Union, British Heart Foundation, Leducq Foundation, Medical Research Council (UK), and German Centre for Cardiovascular Research, from several drug and device companies active in atrial fibrillation, and has received honoraria from several such companies in the past, but not in the last three years. PK is listed as inventor on two patents held by University of Birmingham (Atrial Fibrillation Therapy WO 2015140571, Markers for Atrial Fibrillation WO 2016012783). Andreas Rillig received consultant fees from Medtronic, KODEX-EPD, Biosense Webster and travel grants and lecture fees from Medtronic, Cardiofocus, Biosense Webster, Abbott, Boehringer Ingelheim, Philips KODEX-EPD, Ablamap, Bayer and Novartis.
Figures


References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J. 2021;42:373–498. doi: 10.1093/eurheartj/ehaa612. - DOI - PubMed
-
- Deshmukh A, Patel NJ, Pant S, Shah N, Chothani A, Mehta K, et al. In-hospital complications associated with catheter ablation of atrial fibrillation in the United States between 2000 and 2010: analysis of 93 801 procedures. Circulation. 2013;128:2104–2112. doi: 10.1161/CIRCULATIONAHA.113.003862. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
