

Colorectal cancer screening with fecal immunochemical testing: a community-based, cross-sectional study in average-risk individuals in Nigeria
- PMID: 35714629
- PMCID: PMC9400038
- DOI: 10.1016/S2214-109X(22)00121-8
Colorectal cancer screening with fecal immunochemical testing: a community-based, cross-sectional study in average-risk individuals in Nigeria
Abstract
Background: The estimated incidence of colorectal cancer is rising in Nigeria, where most patients present with advanced disease. Earlier detection of colorectal cancer is a goal of the Nigerian National Cancer Control Plan, but the utility of fecal-based screening is unclear. This study aimed to assess the fecal immunochemical test as a colorectal cancer screening modality in average-risk individualS in Nigeria.
Methods: A population-based, cross-sectional study of qualitative fecal immunochemical test-based colorectal cancer screening was done in asymptomatic, average-risk participants aged 45-75 years in three states in Nigeria (Osun, Kwara, and Lagos). Participants were invited to enrol using age-stratified and sex-stratified convenience sampling following community outreach. Exclusion criteria included a personal history of colorectal cancer or rectal bleeding in the previous 6 months, a first-degree relative with a known diagnosis of colorectal cancer, or a comorbidity that would preclude conscious sedation or general anesthesia. Participants with positive fecal immunochemical test results underwent colonoscopy, and the positive predictive value of fecal immunochemical testing for colorectal cancer and advanced adenomas (≥10 mm, tubulovillous or villous or high-grade dysplasia) was calculated. Data on demographics and acceptability of fecal immunochemical testing and colonoscopy were collected.
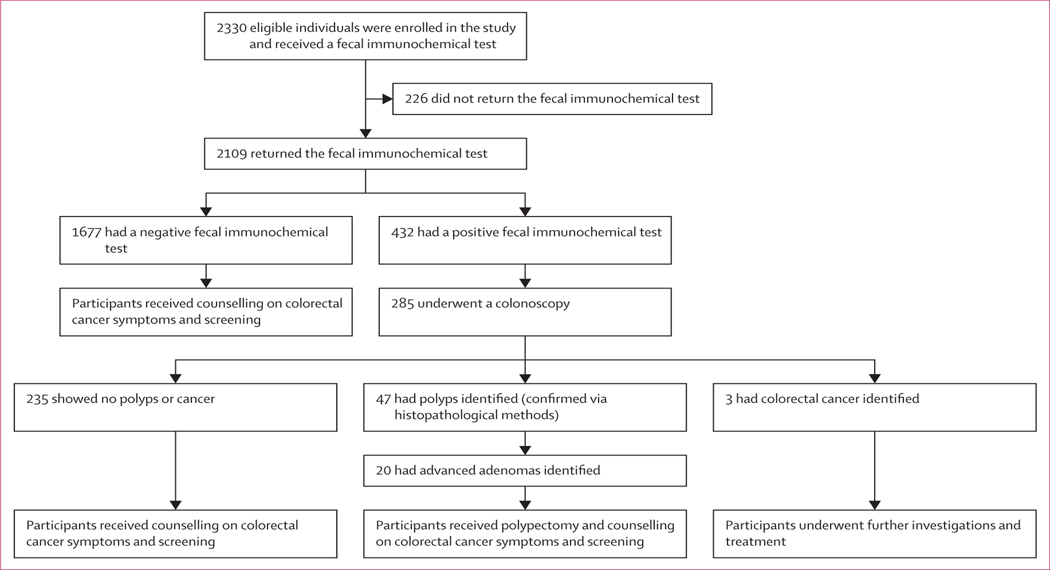
Findings: Between January and April 2021, 2330 participants were enrolled in the study and received a fecal immunochemical test, which was returned by 2109 participants. 1677 participants tested negative and 432 tested positive. Of these 432 participants, 285 underwent a colonoscopy (235 showed no polyps or cancer, 47 had polyps identified, and three had colorectal cancer identified). Of the 47 participants who had polyps identified, 20 had advanced adenomas diagnosed. The median age was 57 years (IQR 50-63), 958 (41%) were male and 1372 (59%) were female, and 68% had at least a secondary-level education. Participants were evenly spread across wealth quintiles. The positivity rate of the fecal immunochemical test was 21% overall (432 of 2109; 95% CI 20-21%), 11% (51 of 455; 95% CI 10-12) in Lagos, 20% (215 of 1052; 95% CI 20-21) in Osun, and 28% (166 of 597; 95% CI 27-29) in Kwara. Among the patients with a positive fecal immunochemical test who completed colonoscopy, the positive predictive value for invasive colorectal cancer was 1·1% (95% CI 0·3-3·3), and 7·0% (4·5-10·8) for advanced adenoma. The acceptability of fecal immunochemical screening among participants was very high.
Interpretation: Colorectal cancer screening with qualitative fecal immunochemical tests in Nigeria is feasible and acceptable to average-risk asymptomatic participants. However, the low positive predictive value for advanced neoplasia and high endoscopy burden investigating false positives suggests it might not be an appropriate screening tool in this setting.
Funding: Thompson Family Foundation, Prevent Cancer Foundation, National Institutes of Health/National Cancer Institute Program Cancer Center.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests TPK reports personal fees from Olympus outside of the submitted work. AJD reports consulting fees from Memorial Sloan Kettering Cancer Center during the conduct of this study. All other authors declare no competing interests.
Comment in
-
Colorectal cancer screening in sub-Saharan Africa.Lancet Glob Health. 2022 Jul;10(7):e938-e939. doi: 10.1016/S2214-109X(22)00231-5. Lancet Glob Health. 2022. PMID: 35714636 No abstract available.
-
Colorectal cancer screening with fecal immunochemical testing in Nigeria.Lancet Glob Health. 2022 Nov;10(11):e1561. doi: 10.1016/S2214-109X(22)00393-X. Lancet Glob Health. 2022. PMID: 36240820 No abstract available.
-
Colorectal cancer screening with fecal immunochemical testing in Nigeria - Authors' reply.Lancet Glob Health. 2022 Nov;10(11):e1562. doi: 10.1016/S2214-109X(22)00404-1. Lancet Glob Health. 2022. PMID: 36240821 No abstract available.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68: 394–424. - PubMed
-
- Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017; 66: 683–91. - PubMed
-
- Cardoso R, Guo F, Heisser T, et al. Colorectal cancer incidence, mortality, and stage distribution in European countries in the colorectal cancer screening era: an international population-based study. Lancet Oncol 2021; 22: 1002–13. - PubMed
-
- Shaukat A, Mongin SJ, Geisser MS, et al. Long-term mortality after screening for colorectal cancer. N Engl J Med 2013; 369: 1106–14. - PubMed
-
- Bray F, Soerjomataram I. The changing global burden of cancer: transitions in human development and implications for cancer prevention and control. In: Gelband H, Jha P, Sankaranarayanan R, Horton S, eds. Cancer: disease control priorities. Third edn (volume 3). Washington (DC: ): The World Bank, 2015. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
