

Incidence of typhoid and paratyphoid fever in Bangladesh, Nepal, and Pakistan: results of the Surveillance for Enteric Fever in Asia Project
- PMID: 35714648
- PMCID: PMC9210262
- DOI: 10.1016/S2214-109X(22)00119-X
Incidence of typhoid and paratyphoid fever in Bangladesh, Nepal, and Pakistan: results of the Surveillance for Enteric Fever in Asia Project
Abstract
Background: Precise enteric fever disease burden data are needed to inform prevention and control measures, including the use of newly available typhoid vaccines. We established the Surveillance for Enteric Fever in Asia Project (SEAP) to inform these strategies.
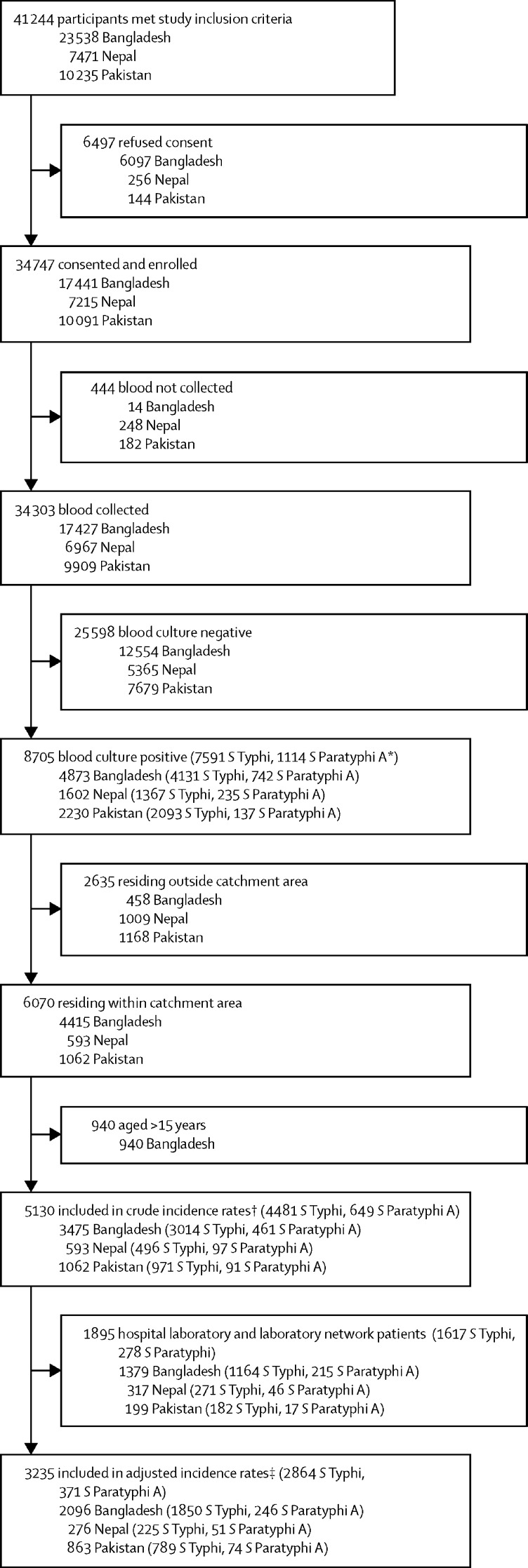
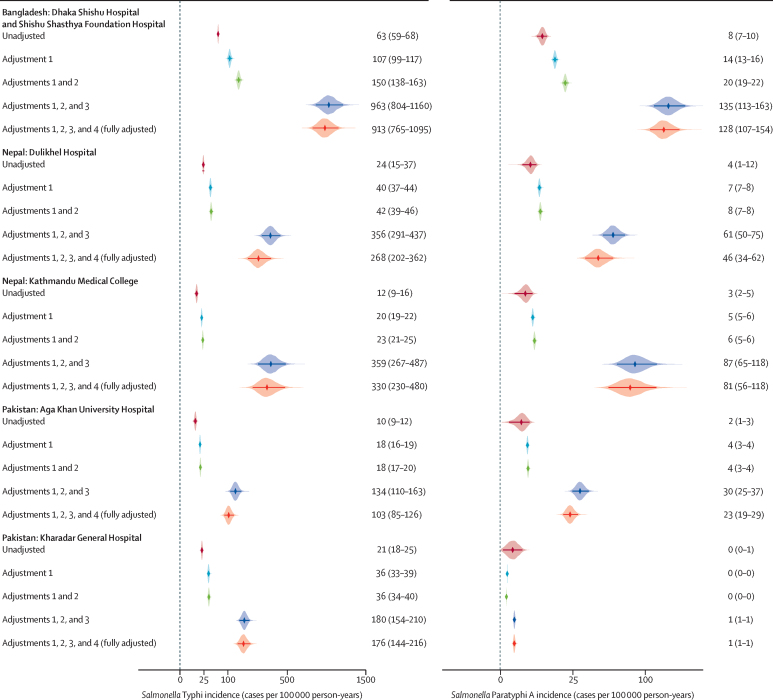
Methods: From September, 2016, to September, 2019, we conducted prospective clinical surveillance for Salmonella enterica serotype Typhi (S Typhi) and Paratyphi (S Paratyphi) A, B, and C at health facilities in predetermined catchment areas in Dhaka, Bangladesh; Kathmandu and Kavrepalanchok, Nepal; and Karachi, Pakistan. Patients eligible for inclusion were outpatients with 3 or more consecutive days of fever in the last 7 days; inpatients with suspected or confirmed enteric fever; patients with blood culture-confirmed enteric fever from the hospital laboratories not captured by inpatient or outpatient enrolment and cases from the laboratory network; and patients with non-traumatic ileal perforation under surgical care. We used a hybrid surveillance model, pairing facility-based blood culture surveillance with community surveys of health-care use. Blood cultures were performed for enrolled patients. We calculated overall and age-specific typhoid and paratyphoid incidence estimates for each study site. Adjusted estimates accounted for the sensitivity of blood culture, the proportion of eligible individuals who consented and provided blood, the probability of care-seeking at a study facility, and the influence of wealth and education on care-seeking. We additionally calculated incidence of hospitalisation due to typhoid and paratyphoid.
Findings: A total of 34 747 patients were enrolled across 23 facilitates (six tertiary hospitals, surgical wards of two additional hospitals, and 15 laboratory network sites) during the study period. Of the 34 303 blood cultures performed on enrolled patients, 8705 (26%) were positive for typhoidal Salmonella. Adjusted incidence rates of enteric fever considered patients in the six tertiary hospitals. Adjusted incidence of S Typhi, expressed per 100 000 person-years, was 913 (95% CI 765-1095) in Dhaka. In Nepal, the adjusted typhoid incidence rates were 330 (230-480) in Kathmandu and 268 (202-362) in Kavrepalanchok. In Pakistan, the adjusted incidence rates per hospital site were 176 (144-216) and 103 (85-126). The adjusted incidence rates of paratyphoid (of which all included cases were due to S Paratyphi A) were 128 (107-154) in Bangladesh, 46 (34-62) and 81 (56-118) in the Nepal sites, and 23 (19-29) and 1 (1-1) in the Pakistan sites. Adjusted incidence of hospitalisation was high across sites, and overall, 2804 (32%) of 8705 patients with blood culture-confirmed enteric fever were hospitalised.
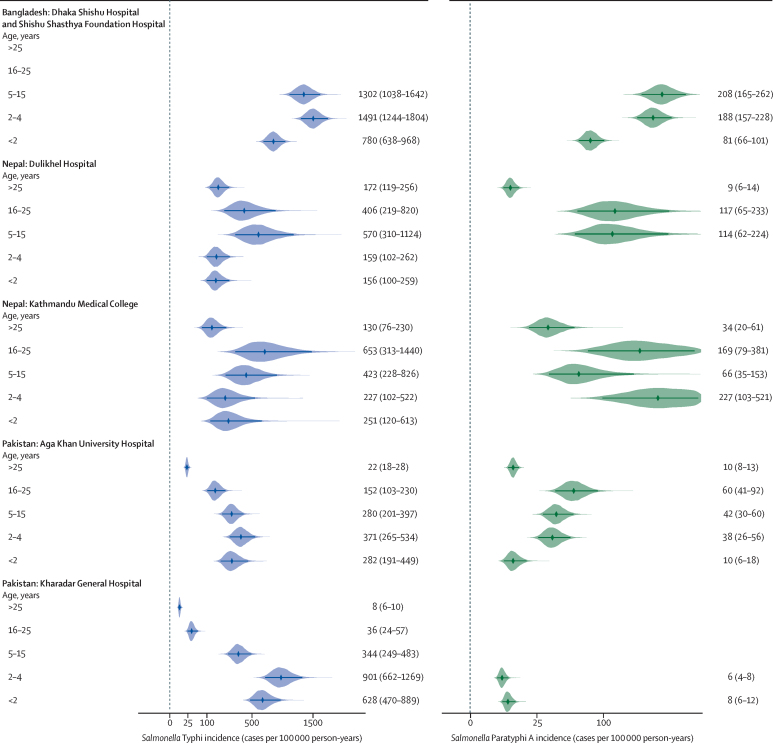
Interpretation: Across diverse communities in three south Asian countries, adjusted incidence exceeded the threshold for "high burden" of enteric fever (100 per 100 000 person-years). Incidence was highest among children, although age patterns differed across sites. The substantial disease burden identified highlights the need for control measures, including improvements to water and sanitation infrastructure and the implementation of typhoid vaccines.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Tackling typhoid fever burden in south Asia.Lancet Glob Health. 2022 Jul;10(7):e932-e933. doi: 10.1016/S2214-109X(22)00210-8. Lancet Glob Health. 2022. PMID: 35714634 No abstract available.
References
-
- Karkey A, Thwaites GE, Baker S. The evolution of antimicrobial resistance in Salmonella Typhi. Curr Opin Gastroenterol. 2018;34:25–30. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
