

Low-molecular-weight heparin compared with unfractionated heparin in critically ill COVID-19 patients
- PMID: 35716998
- PMCID: PMC9212478
- DOI: 10.1016/j.jvsv.2022.04.019
Low-molecular-weight heparin compared with unfractionated heparin in critically ill COVID-19 patients
Abstract
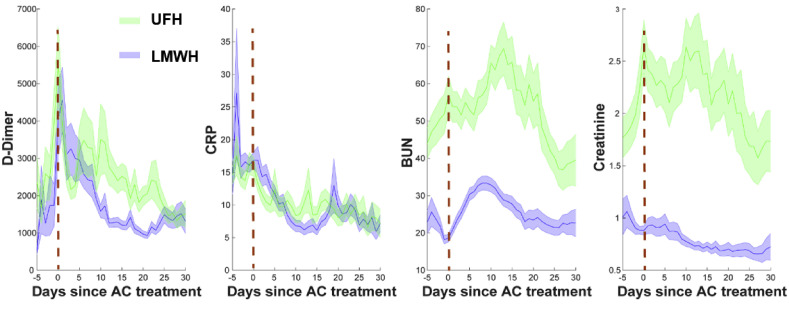
Background: Thrombosis in COVID-19 worsens mortality. In our study, we sought to investigate how the dose and type of anticoagulation (AC) can influence patient outcomes.
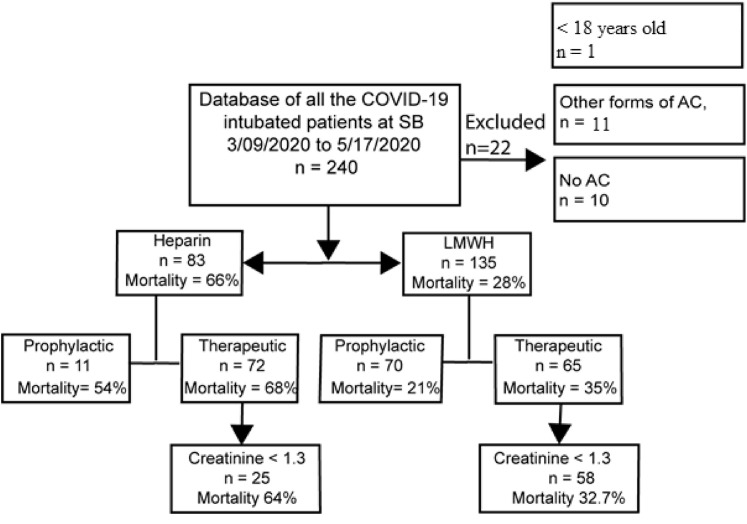
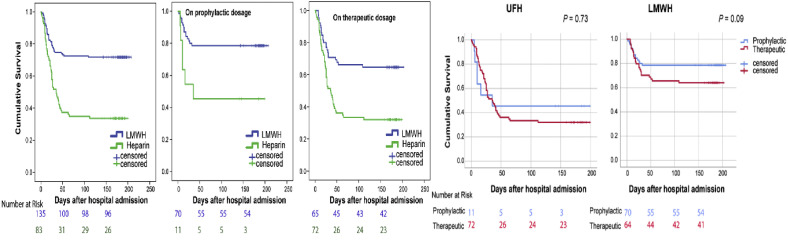
Methods: This is a single-center retrospective analysis of critically ill intubated patients with COVID-19, comparing low-molecular-weight heparin (LMWH) and unfractionated heparin (UFH) at therapeutic and prophylactic doses. Of 218 patients, 135 received LMWH (70 prophylactic, 65 therapeutic) and 83 UFH (11 prophylactic, 72 therapeutic). The primary outcome was mortality. Secondary outcomes were thromboembolic complications confirmed on imaging and major bleeding complications. Cox proportional-hazards regression models were used to determine whether the type and dose of AC were independent predictors of survival. We performed Kaplan-Meier survival analysis to compare the cumulative survivals.
Results: Overall, therapeutic AC, with either LMWH (65% vs 79%, P = .09) or UFH (32% vs 46%, P = .73), conveyed no survival benefit over prophylactic AC. UFH was associated with a higher mortality rate than LMWH (66% vs 28%, P = .001), which was also evident in the multivariable analysis (LMWH vs UFH mortality, hazard ratio: 0.47, P = .001) and in the Kaplan-Meier survival analysis. Thrombotic and bleeding complications did not depend on the AC type (prophylactic LMWH vs UFH: thrombosis P = .49, bleeding P = .075; therapeutic LMWH vs UFH: thrombosis P = .5, bleeding P = .17). When comparing prophylactic with therapeutic AC, the rate of both thrombotic and bleeding complications was higher with the use of LMWH compared with UFH. In addition, transfusion requirements were significantly higher with both therapeutic LMWH and UFH.
Conclusions: Among intubated critically ill COVID-19 intensive care unit patients, therapeutic AC, with either LMWH or UFH, conveyed no survival benefit over prophylactic AC. AC with LMWH was associated with higher cumulative survival compared with AC with UFH.
Keywords: Anticoagulation (AC); COVID-19; Low-molecular-weight heparin (LMWH); SARS-CoV-2; Thromboprophylaxis; Unfractionated heparin (UFH).
Published by Elsevier Inc.
Figures
References
-
- Worldometer. https://www.worldometers.info/coronavirus/
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
