

The association between ambient UVB dose and ANCA-associated vasculitis relapse and onset
- PMID: 35717248
- PMCID: PMC9206351
- DOI: 10.1186/s13075-022-02834-6
The association between ambient UVB dose and ANCA-associated vasculitis relapse and onset
Abstract
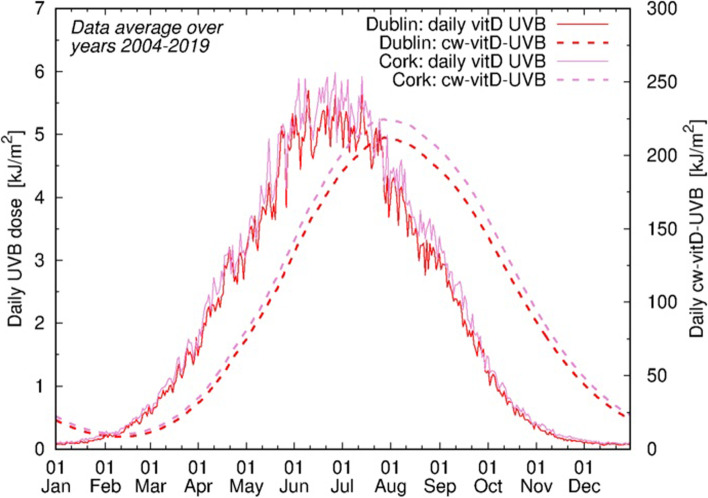
Background: The aetiology of ANCA-associated vasculitis (AAV) and triggers of relapse are poorly understood. Vitamin D (vitD) is an important immunomodulator, potentially responsible for the observed latitudinal differences between granulomatous and non-granulomatous AAV phenotypes. A narrow ultraviolet B spectrum induces vitD synthesis (vitD-UVB) via the skin. We hypothesised that prolonged periods of low ambient UVB (and by extension vitD deficiency) are associated with the granulomatous form of the disease and an increased risk of AAV relapse.
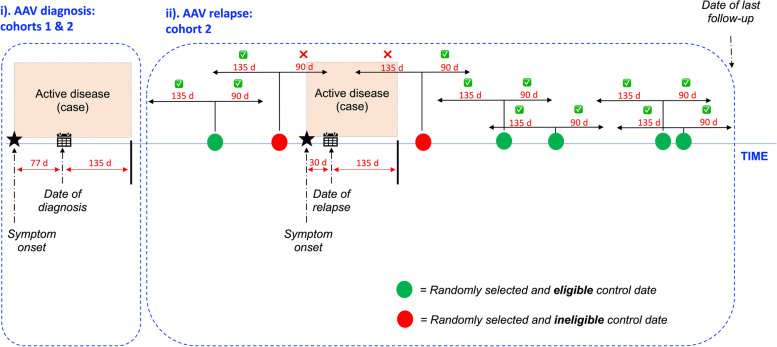
Methods: Patients with AAV recruited to the Irish Rare Kidney Disease (RKD) (n = 439) and UKIVAS (n = 1961) registries were studied. Exposure variables comprised latitude and measures of ambient vitD-UVB, including cumulative weighted UVB dose (CW-D-UVB), a well-validated vitD proxy. An n-of-1 study design was used to examine the relapse risk using only the RKD dataset. Multi-level models and logistic regression were used to examine the effect of predictors on AAV relapse risk, phenotype and serotype.
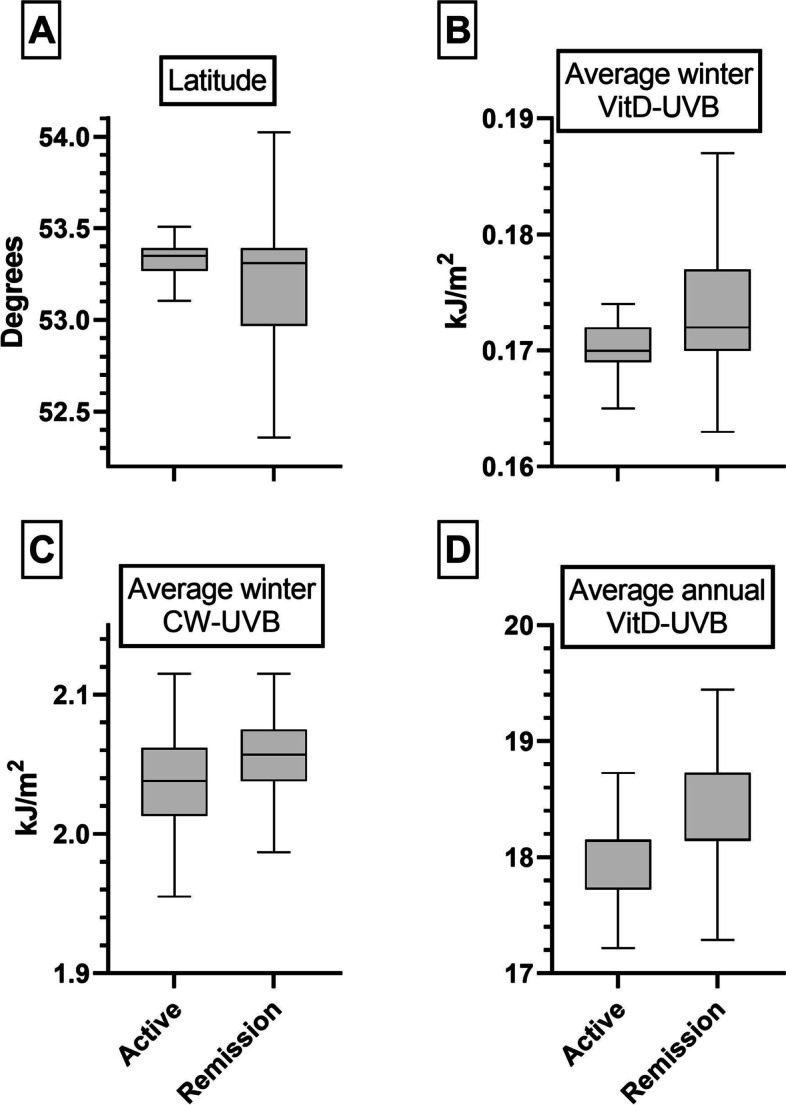
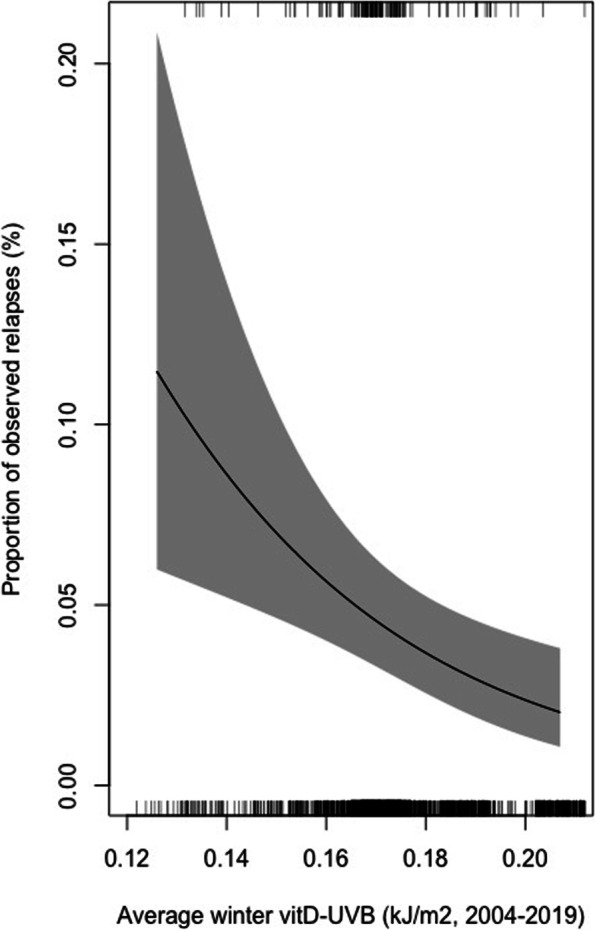
Results: Residential latitude was positively correlated (OR 1.41, 95% CI 1.14-1.74, p = 0.002) and average vitD-UVB negatively correlated (0.82, 0.70-0.99, p = 0.04) with relapse risk, with a stronger effect when restricting to winter measurements (0.71, 0.57-0.89, p = 0.002). However, these associations were not restricted to granulomatous phenotypes. We observed no clear relationship between latitude, vitD-UVB or CW-D-UVB and AAV phenotype or serotype.
Conclusion: Our findings suggest that low winter ambient UVB and prolonged vitD status contribute to AAV relapse risk across all phenotypes. However, the development of a granulomatous phenotype does not appear to be directly vitD-mediated. Further research is needed to determine whether sufficient vitD status would reduce relapse propensity in AAV.
Keywords: ANCA-associated vasculitis; Environment; Geoepidemiology; Ultraviolet B (UVB) radiation; Vitamin D.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
