

Long-term cardiac surveillance and outcomes of COVID-19 patients
- PMID: 35718289
- PMCID: PMC9212847
- DOI: 10.1016/j.tcm.2022.06.003
Long-term cardiac surveillance and outcomes of COVID-19 patients
Abstract
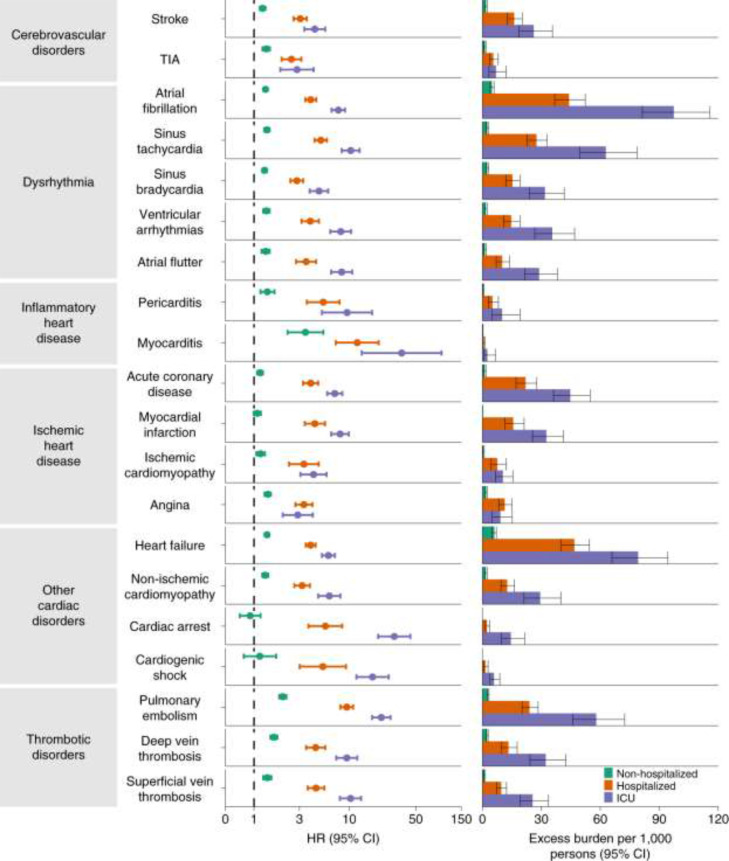
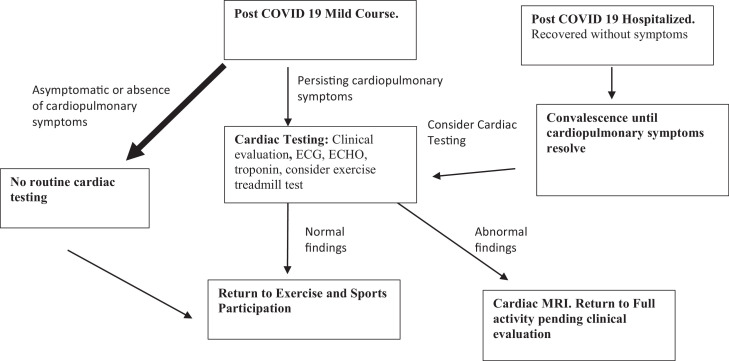
Acute cardiac manifestions of COVID-19 have been well described, while chronic cardiac sequelae remain less clear. Various studies have shown conflicting data on the prevalence of new or worsening cardiovascular disease, myocarditis or cardiac dysrhythmias among patients recovered from COVID-19. Data are emerging that show that patients recovering from COVID-19 have an increased incidence of myocarditis and arrhythmias after recovery from COVID-19 compared with the control groups without COVID-19. The incidence of myocarditis after COVID-19 infection is low but is still significantly greater than the incidence of myocarditis from a COVID-19 vaccine. There have been several studies of athletes who underwent a variety of screening protocols prior to being cleared to return to exercise and competition. The data show possible, probable or definite myocarditis or cardiac injury among 0.4-3.0% of the athletes studied. Recent consensus statements suggest that athletes with full recovery and absence of cardiopulmonary symptoms may return to exercise and competition without cardiovascular testing. In conclusion, patients with COVID-19 may be expected to have an increased risk of cardiovascular disease, myocarditis or arrhythmias during the convalescent phase. Fortunately, the majority of patients, including athletes may return to their normal activity after recovery from COVID 19, in the absence of persisting cardiovascular symptoms.
Copyright © 2022. Published by Elsevier Inc.
Figures
Comment in
-
Editorial commentary: COVID-19 as a cardiovascular disease risk factor.Trends Cardiovasc Med. 2022 Nov;32(8):476-478. doi: 10.1016/j.tcm.2022.07.003. Epub 2022 Jul 16. Trends Cardiovasc Med. 2022. PMID: 35850405 Free PMC article. No abstract available.
References
-
- Wiersinga W.J., Rhodes A., Cheng A.C., Peacock S.J., Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;324:782–793. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
