

A Single-Cell Atlas of Tumor-Infiltrating Immune Cells in Pancreatic Ductal Adenocarcinoma
- PMID: 35718340
- PMCID: PMC9294203
- DOI: 10.1016/j.mcpro.2022.100258
A Single-Cell Atlas of Tumor-Infiltrating Immune Cells in Pancreatic Ductal Adenocarcinoma
Abstract
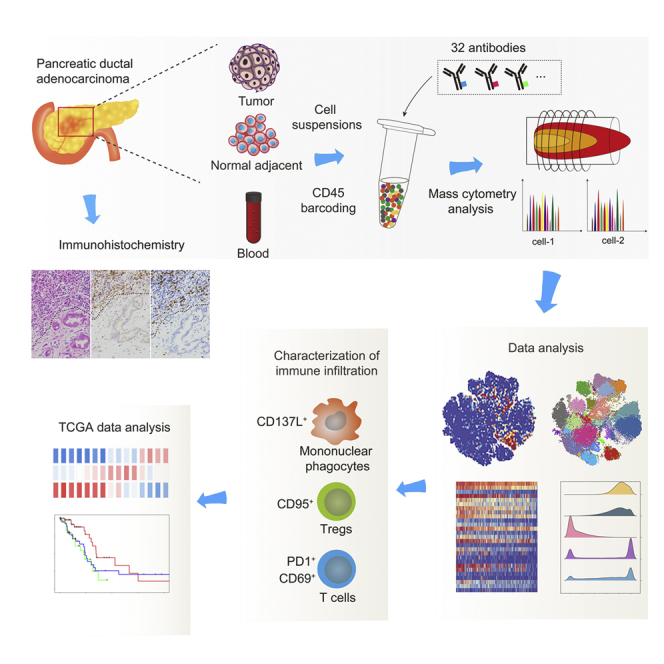
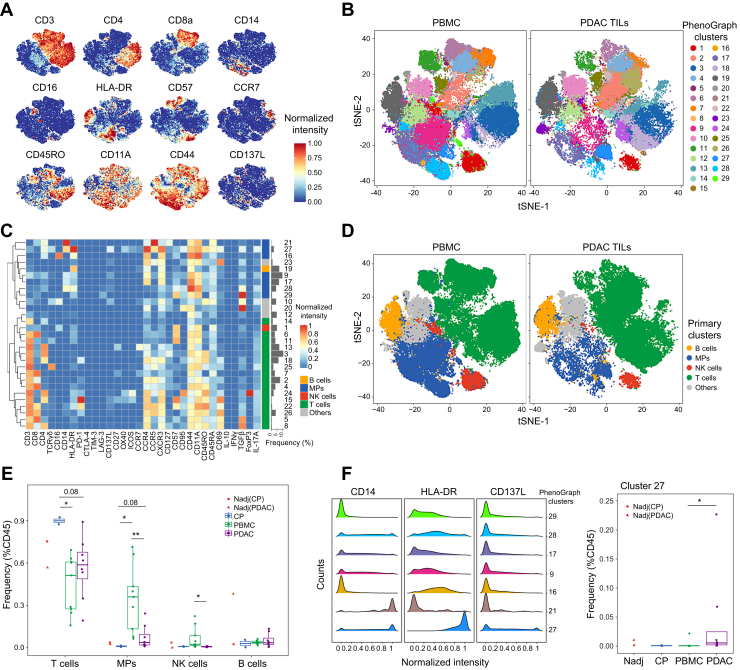
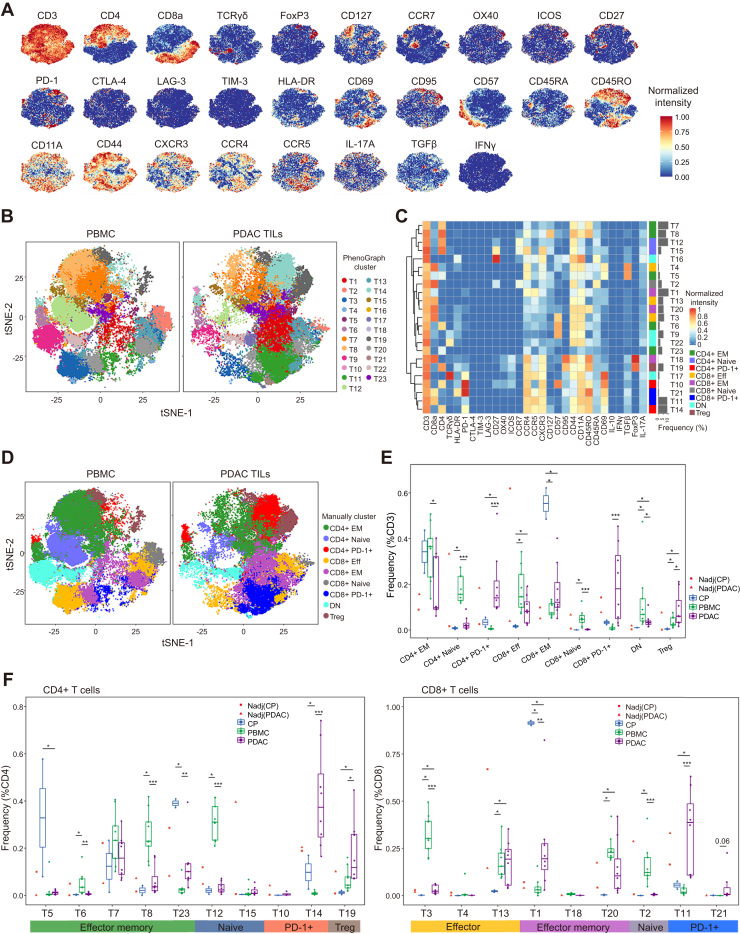
Pancreatic ductal adenocarcinoma (PDAC) is one of the most lethal malignancies with limited treatment options. To guide the design of more effective immunotherapy strategies, mass cytometry was employed to characterize the cellular composition of the PDAC-infiltrating immune cells. The expression of 33 protein markers was examined at the single-cell level in more than two million immune cells from four types of clinical samples, including PDAC tumors, normal pancreatic tissues, chronic pancreatitis tissues, and peripheral blood. Based on the analyses, we identified 23 distinct T-cell phenotypes, with some cell clusters exhibiting aberrant frequencies in the tumors. Programmed cell death protein 1 (PD-1) was extensively expressed in CD4+ and CD8+ T cells and coexpressed with both stimulatory and inhibitory immune markers. In addition, we observed elevated levels of functional markers, such as CD137L and CD69, in PDAC-infiltrating immune cells. Moreover, the combination of PD-1 and CD8 was used to stratify PDAC tumors from The Cancer Genome Atlas database into three immune subtypes, with S1 (PD-1+CD8+) exhibiting the best prognosis. Further analysis suggested distinct molecular mechanisms for immune exclusion in different subtypes. Taken together, the single-cell protein expression data depicted a detailed cell atlas of the PDAC-infiltrating immune cells and revealed clinically relevant information regarding useful cell phenotypes and targets for immunotherapy development.
Keywords: cancer immunology; mass cytometry; pancreatic ductal adenocarcinoma; single-cell analysis; tumor microenvironment.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest The authors declare no competing interests.
Figures




References
-
- Kleeff J., Korc M., Apte M., La Vecchia C., Johnson C.D., Biankin A.V., et al. Pancreatic cancer. Nat. Rev. Dis. Primers. 2016;2 - PubMed
-
- Rahib L., Smith B.D., Aizenberg R., Rosenzweig A.B., Fleshman J.M., Matrisian L.M. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–2921. - PubMed
-
- Bailey P., Chang D.K., Nones K., Johns A.L., Patch A.M., Gingras M.C., et al. Genomic analyses identify molecular subtypes of pancreatic cancer. Nature. 2016;531:47–52. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
