

Lesion Localization and Prognosis Using Electrodiagnostic Studies in Facial Diplegia: A Rare Variant of Guillain-Barre Syndrome
- PMID: 35719795
- PMCID: PMC9200109
- DOI: 10.7759/cureus.25047
Lesion Localization and Prognosis Using Electrodiagnostic Studies in Facial Diplegia: A Rare Variant of Guillain-Barre Syndrome
Abstract
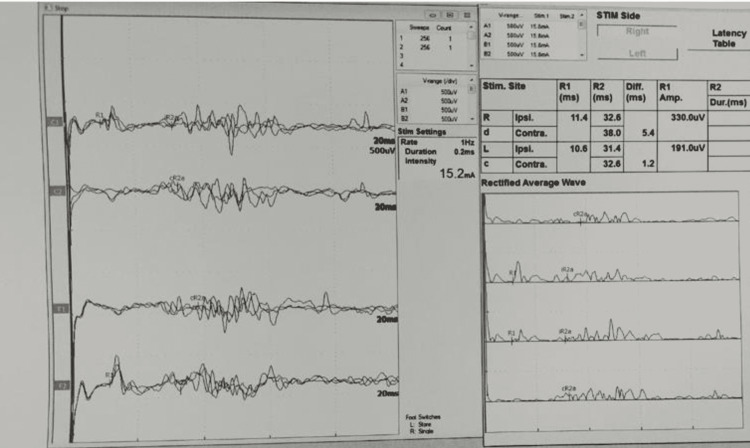
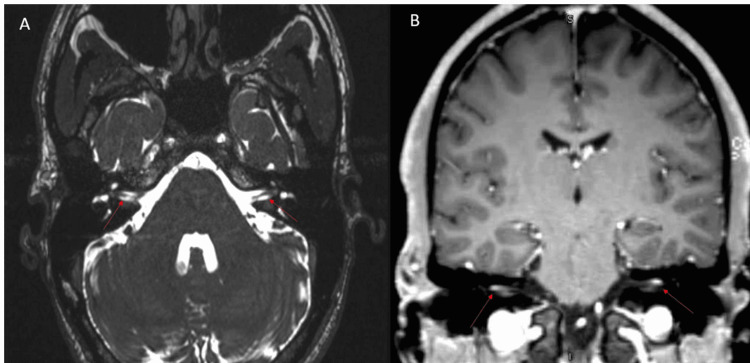
Background The etiology of facial nerve palsy is diverse and includes herpes zoster virus, Guillain-Barre syndrome (GBS), otitis media, Lyme disease, sarcoidosis, human immunodeficiency virus, etc. The lower motor neuron type facial nerve palsy is usually caused by an ipsilateral facial nerve lesion; however, it may be caused by a central lesion of the facial nerve nucleus and tract in the pons. Facial diplegia is an extremely rare condition that occurs in approximately 0.3% to 2.0% of all facial palsies. Electrodiagnostic studies including direct facial nerve conduction, facial electromyography (EMG), and blink reflex studies are useful for the prognosis and lesion localization in facial nerve palsy. Methodology This retrospective, observational study was conducted at the Neurophysiology Unit, Hamad General Hospital, Doha, Qatar. This study included 11 patients with bilateral facial weakness who visited for electrodiagnostic studies in the neurophysiology laboratory. Results In total, eight (72.7%) patients had facial diplegia, eight (72.7%) had hypo/areflexia, seven (63.6%) had facial numbness, and five (45.5%) had cerebrospinal fluid albuminocytological dissociation. The most frequent cause of facial diplegia in this study was GBS (81.9%). Direct facial nerve conduction stimulation showed that nine (81.8%) patients had bilateral facial nerve low compound muscle action potential amplitudes. The bilateral blink reflex study showed that eight (88.8%) patients had absent bilateral evoked responses. Finally, the EMG study showed that five (55.5%) patients had active denervation in bilateral sample facial muscles. Conclusions Bilateral facial nerve palsy is an extremely rare condition with a varied etiology. Electrodiagnostic studies are useful in detecting the underlying pathophysiologic processes, prognosis, and central or peripheral lesion localization in patients with facial diplegia.
Keywords: acute motor axonal neuropathy (aman); amplitude degeneration index (adi); facial diplegia (fd); guillain-barre syndrome (gbs); nerve conduction study (ncs).
Copyright © 2022, Ali et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- The facial nerve. Current trends in diagnosis, treatment, and rehabilitation. Jackson CG, von Doersten PG. Med Clin North Am. 1999;83:179-95, x. - PubMed
-
- Differential diagnosis of facial nerve palsy. May M, Klein SR. Otolaryngol Clin North Am. 1991;24:613–645. - PubMed
-
- Natural history of Bell's palsy. Peitersen E. Acta Otolaryngol Suppl. 1992;492:122–124. - PubMed
-
- Idiopathic facial paralysis, pregnancy, and the menstrual cycle. Hilsinger RL Jr, Adour KK, Doty HE. Ann Otol Rhinol Laryngol. 1975;84:433–442. - PubMed
LinkOut - more resources
Full Text Sources